University of Oxford Centre for Clinical Magnetic Resonance Research, Department of Cardiovascular Medicine, John Radcliffe Hospital, Oxford, UK.
J Cardiovasc Magn Reson. 2010 Nov 19;12(1):69. doi: 10.1186/1532-429X-12-69.
T1 mapping allows direct in-vivo quantitation of microscopic changes in the myocardium, providing new diagnostic insights into cardiac disease. Existing methods require long breath holds that are demanding for many cardiac patients. In this work we propose and validate a novel, clinically applicable, pulse sequence for myocardial T1-mapping that is compatible with typical limits for end-expiration breath-holding in patients.
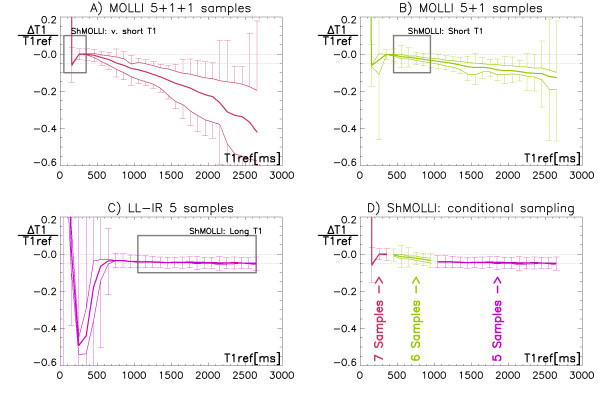
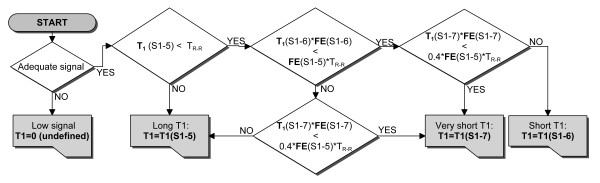
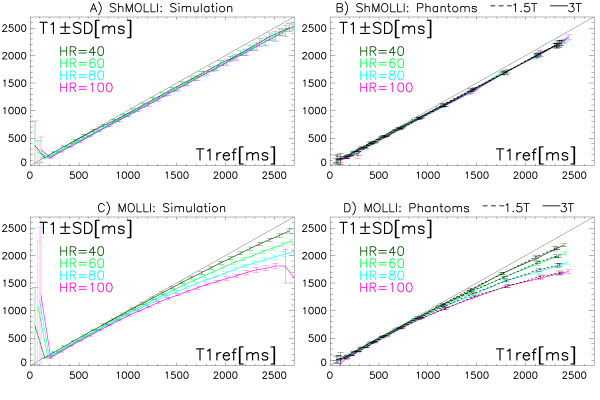
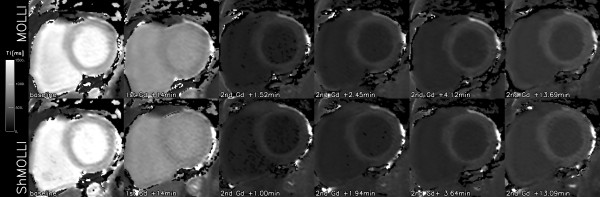
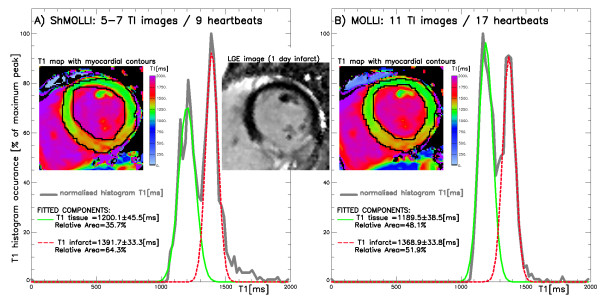
The Shortened MOdified Look-Locker Inversion recovery (ShMOLLI) method uses sequential inversion recovery measurements within a single short breath-hold. Full recovery of the longitudinal magnetisation between sequential inversion pulses is not achieved, but conditional interpretation of samples for reconstruction of T1-maps is used to yield accurate measurements, and this algorithm is implemented directly on the scanner. We performed computer simulations for 100 ms<T1 < 2.7 s and heart rates 40-100 bpm followed by phantom validation at 1.5T and 3T. In-vivo myocardial T1-mapping using this method and the previous gold-standard (MOLLI) was performed in 10 healthy volunteers at 1.5T and 3T, 4 volunteers with contrast injection at 1.5T, and 4 patients with recent myocardial infarction (MI) at 3T.
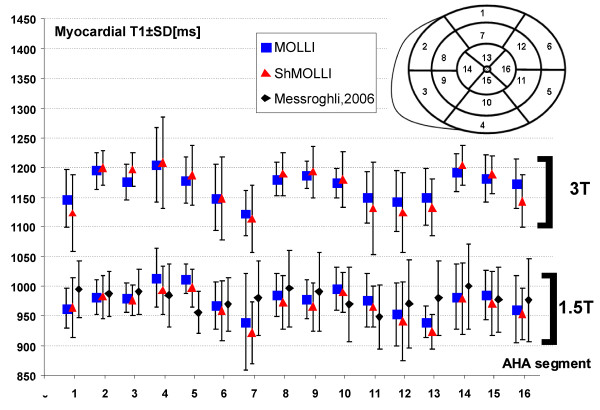
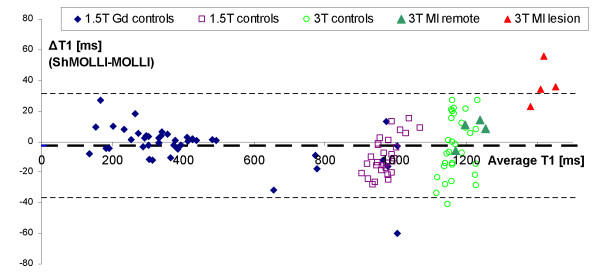
We found good agreement between the average ShMOLLI and MOLLI estimates for T1 < 1200 ms. In contrast to the original method, ShMOLLI showed no dependence on heart rates for long T1 values, with estimates characterized by a constant 4% underestimation for T1 = 800-2700 ms. In-vivo, ShMOLLI measurements required 9.0 ± 1.1 s (MOLLI = 17.6 ± 2.9 s). Average healthy myocardial T1 s by ShMOLLI at 1.5T were 966 ± 48 ms (mean ± SD) and 1166 ± 60 ms at 3T. In MI patients, the T1 in unaffected myocardium (1216 ± 42 ms) was similar to controls at 3T. Ischemically injured myocardium showed increased T1 = 1432 ± 33 ms (p < 0.001). The difference between MI and remote myocardium was estimated 15% larger by ShMOLLI than MOLLI (p < 0.04) which suffers from heart rate dependencies for long T1. The in-vivo variability within ShMOLLI T1-maps was only 14% (1.5T) or 18% (3T) higher than the MOLLI maps, but the MOLLI acquisitions were twice longer than ShMOLLI acquisitions.
ShMOLLI is an efficient method that generates immediate, high-resolution myocardial T1-maps in a short breath-hold with high precision. This technique provides a valuable clinically applicable tool for myocardial tissue characterisation.
T1 映射允许对心肌的微观变化进行直接体内定量,为心脏疾病的诊断提供新的见解。现有的方法需要长时间的屏气,这对许多心脏病患者来说是很苛刻的。在这项工作中,我们提出并验证了一种新的、临床适用的心肌 T1 映射脉冲序列,该序列与患者呼气末屏气的典型限制兼容。
缩短的改良 Look-Locker 反转恢复(ShMOLLI)方法在单次短屏气中使用连续的反转恢复测量。在连续的反转脉冲之间,纵向磁化没有完全恢复,但使用条件解释样本来重建 T1 图谱,以获得准确的测量结果,并且该算法直接在扫描仪上实现。我们对 100ms<T1<2.7s 和心率 40-100bpm 进行了计算机模拟,然后在 1.5T 和 3T 进行了体模验证。在 1.5T 和 3T 对 10 名健康志愿者、4 名在 1.5T 接受对比剂注射的志愿者和 4 名患有近期心肌梗死(MI)的患者进行了基于 ShMOLLI 和以前的金标准(MOLLI)的心肌 T1 映射。
我们发现 ShMOLLI 和 MOLLI 对 T1<1200ms 的平均估计值之间有很好的一致性。与原始方法不同,ShMOLLI 对长 T1 值没有心率依赖性,其特征是 T1=800-2700ms 时的估计值恒定低估 4%。在体内,ShMOLLI 测量需要 9.0±1.1s(MOLLI=17.6±2.9s)。ShMOLLI 在 1.5T 时的平均健康心肌 T1s 为 966±48ms(平均值±标准差),在 3T 时为 1166±60ms。在 MI 患者中,未受影响心肌的 T1(1216±42ms)在 3T 时与对照组相似。缺血性损伤心肌的 T1 增加到 1432±33ms(p<0.001)。ShMOLLI 比 MOLLI 估计的 MI 和远隔心肌之间的差异大 15%(p<0.04),MOLLI 受长 T1 的心率依赖性影响。ShMOLLI 内 T1 图谱的体内变异性仅比 MOLLI 图谱高 14%(1.5T)或 18%(3T),但 MOLLI 采集比 ShMOLLI 采集长两倍。
ShMOLLI 是一种高效的方法,可在短屏气中生成即时、高分辨率的心肌 T1 图谱,具有高精度。该技术为心肌组织特征提供了一种有价值的临床适用工具。