Department of Critical Care Medicine, University of Pittsburgh Medical Center, 230 Lothrop Street, Pittsburgh, PA 15261, USA.
Crit Care. 2010;14(6):R212. doi: 10.1186/cc9335. Epub 2010 Nov 23.
Although less invasive than pulmonary artery catheters (PACs), arterial pulse pressure analysis techniques for estimating cardiac output (CO) have not been simultaneously compared to PAC bolus thermodilution CO (COtd) or continuous CO (CCO) devices.
We compared the accuracy, bias and trending ability of LiDCO™, PiCCO™ and FloTrac™ with PACs (COtd, CCO) to simultaneously track CO in a prospective observational study in 17 postoperative cardiac surgery patients for the first 4 hours following intensive care unit admission. Fifty-five paired simultaneous quadruple CO measurements were made before and after therapeutic interventions (volume, vasopressor/dilator, and inotrope).
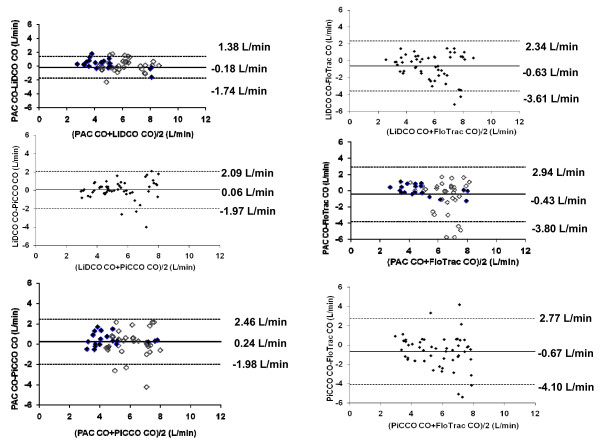
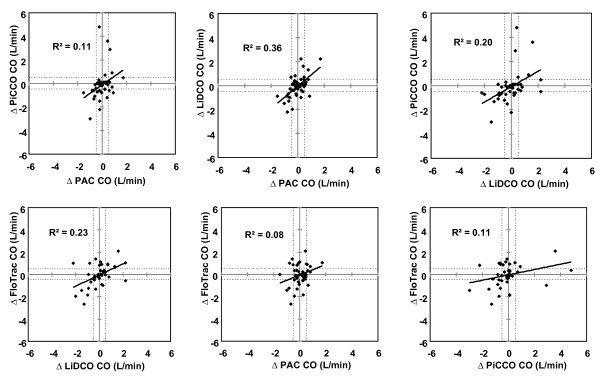
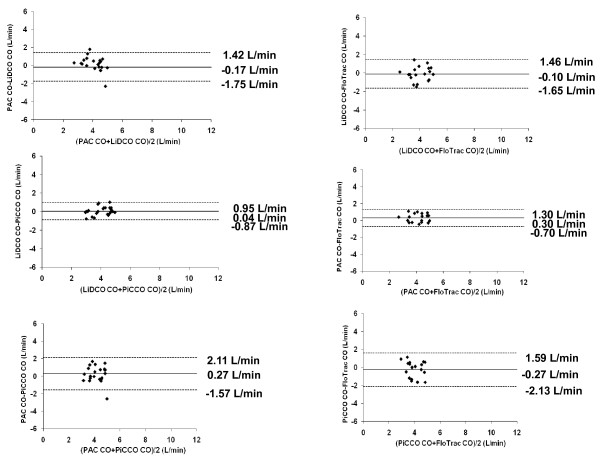
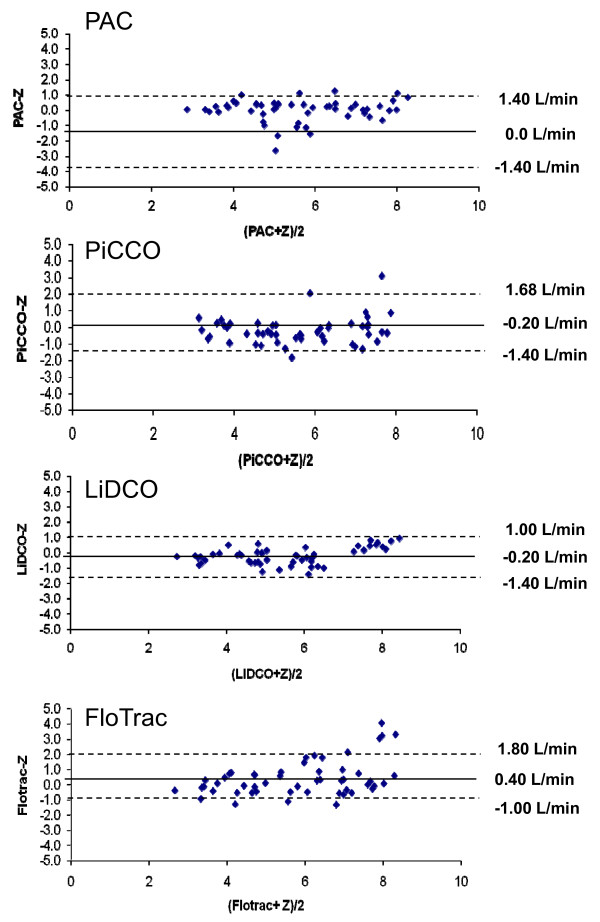
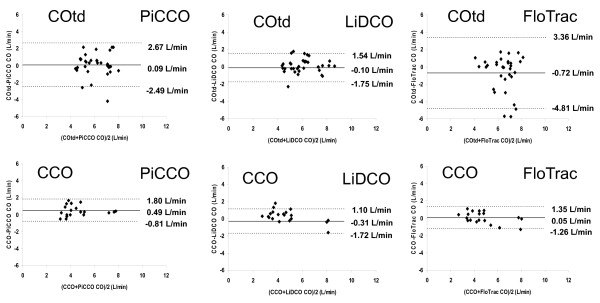
Mean CO values for PAC, LiDCO, PiCCO and FloTrac were similar (5.6 ± 1.5, 5.4 ± 1.6, 5.4 ± 1.5 and 6.1 ± 1.9 L/min, respectively). The mean CO bias by each paired method was -0.18 (PAC-LiDCO), 0.24 (PAC-PiCCO), -0.43 (PAC-FloTrac), 0.06 (LiDCO-PiCCO), -0.63 (LiDCO-FloTrac) and -0.67 L/min (PiCCO-FloTrac), with limits of agreement (1.96 standard deviation, 95% confidence interval) of ± 1.56, ± 2.22, ± 3.37, ± 2.03, ± 2.97 and ± 3.44 L/min, respectively. The instantaneous directional changes between any paired CO measurements displayed 74% (PAC-LiDCO), 72% (PAC-PiCCO), 59% (PAC-FloTrac), 70% (LiDCO-PiCCO), 71% (LiDCO-FloTrac) and 63% (PiCCO-FloTrac) concordance, but poor correlation (r(2) = 0.36, 0.11, 0.08, 0.20, 0.23 and 0.11, respectively). For mean CO < 5 L/min measured by each paired devices, the bias decreased slightly.
Although PAC (COTD/CCO), FloTrac, LiDCO and PiCCO display similar mean CO values, they often trend differently in response to therapy and show different interdevice agreement. In the clinically relevant low CO range (< 5 L/min), agreement improved slightly. Thus, utility and validation studies using only one CO device may potentially not be extrapolated to equivalency of using another similar device.
虽然动脉脉搏压分析技术(用于估计心输出量(CO))比肺动脉导管(PACs)的侵入性小,但尚未同时将其与 PAC 热稀释 CO(COtd)或连续 CO(CCO)设备进行比较。
我们比较了 LiDCO™、PiCCO™ 和 FloTrac™与 PAC(COtd、CCO)的准确性、偏差和趋势能力,在 17 例心脏手术后患者入重症监护病房后 4 小时内进行了前瞻性观察研究。在治疗干预(容量、血管加压药/扩张剂和正性肌力药)前后进行了 55 次同时的四重 CO 测量。
PAC、LiDCO、PiCCO 和 FloTrac 的平均 CO 值相似(分别为 5.6±1.5、5.4±1.6、5.4±1.5 和 6.1±1.9 L/min)。每个配对方法的平均 CO 偏差为-0.18(PAC-LiDCO)、0.24(PAC-PiCCO)、-0.43(PAC-FloTrac)、0.06(LiDCO-PiCCO)、-0.63(LiDCO-FloTrac)和-0.67 L/min(PiCCO-FloTrac),其一致性范围(1.96 标准差,95%置信区间)分别为±1.56、±2.22、±3.37、±2.03、±2.97 和±3.44 L/min。任何配对 CO 测量之间的即时方向变化显示 74%(PAC-LiDCO)、72%(PAC-PiCCO)、59%(PAC-FloTrac)、70%(LiDCO-PiCCO)、71%(LiDCO-FloTrac)和 63%(PiCCO-FloTrac)一致性,但相关性差(r²=0.36、0.11、0.08、0.20、0.23 和 0.11)。对于每个配对设备测量的平均 CO <5 L/min,偏差略有减小。
尽管 PAC(COtd/CCO)、FloTrac、LiDCO 和 PiCCO 显示出相似的平均 CO 值,但它们在对治疗的反应中往往表现出不同的趋势,并且显示出不同的设备间一致性。在临床相关的低 CO 范围(<5 L/min)中,一致性略有改善。因此,仅使用一种 CO 设备的效用和验证研究可能无法推断使用另一种类似设备的等效性。