Institute of Cancer Research, Royal Marsden NHS Foundation Trust, London, UK.
Lancet. 2010 Dec 11;376(9757):1989-99. doi: 10.1016/S0140-6736(10)62051-X. Epub 2010 Dec 3.
Bisphosphonates reduce the risk of skeletal events in patients with malignant bone disease, and zoledronic acid has shown potential anticancer effects in preclinical and clinical studies. We aimed to establish whether bisphosphonates can affect clinical outcomes in patients with multiple myeloma.
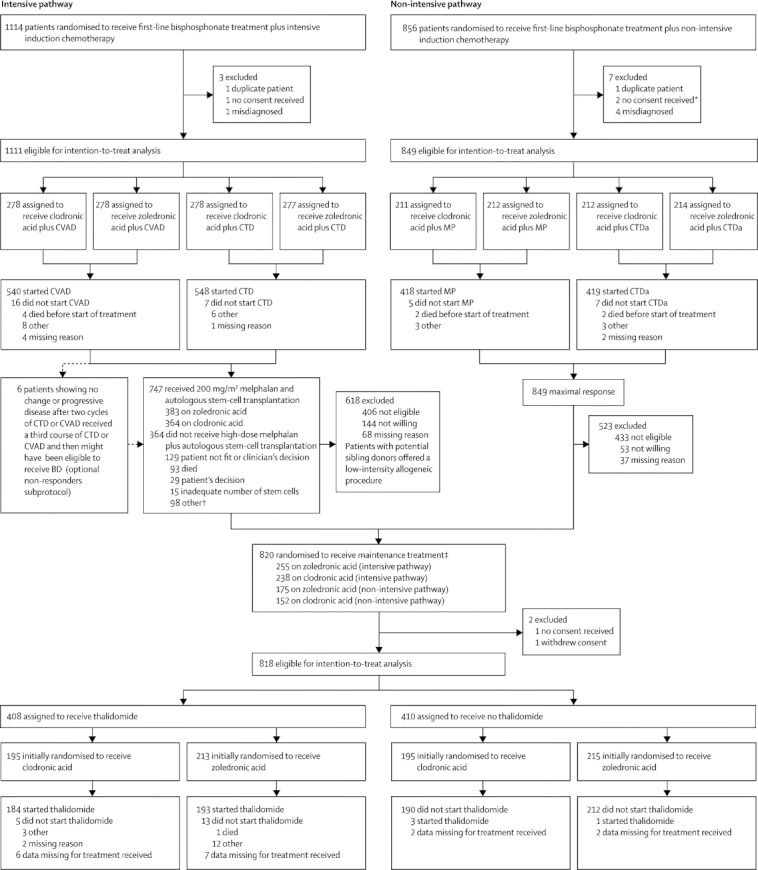
Patients of age 18 years or older with newly diagnosed multiple myeloma were enrolled from 120 centres in the UK. Computer-generated randomisation sequence was used to allocate patients equally, via an automated telephone service, to receive 4 mg zoledronic acid as an infusion every 3-4 weeks or 1600 mg oral clodronic acid daily. Patients also received intensive or non-intensive induction chemotherapy. No investigators, staff, or patients were masked to treatment allocation, and bisphosphonate and maintenance therapy continued at least until disease progression. The primary endpoints were overall survival, progression-free survival, and overall response rate. We assessed between-group differences with Cox proportional hazards models for progression-free survival and overall survival, and with logistic regression models for overall response rate. Analysis was by intention to treat. This trial is registered, number ISRCTN68454111.
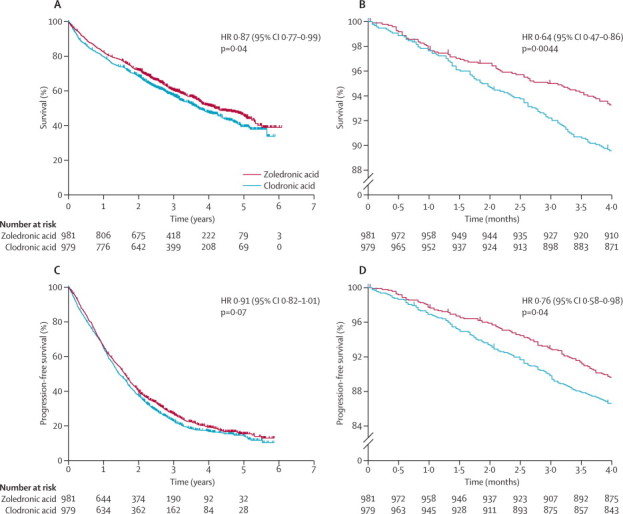
1970 patients were enrolled between May, 2003, and November, 2007, of whom 1960 were eligible for intention-to-treat analysis: 981 in the zoledronic acid group (555 on intensive chemotherapy, 426 on non-intensive chemotherapy); and 979 on clodronic acid (556 on intensive chemotherapy, 423 on non-intensive chemotherapy). The treatment cutoff was Oct 5, 2009, with patients receiving bisphosphonates for a median of 350 days (IQR 137-632) before disease progression, with a median of 3·7 years' follow-up (IQR 2·9-4·7). Zoledronic acid reduced mortality by 16% (95% CI 4-26) versus clodronic acid (hazard ratio [HR] 0·84, 95% CI 0·74-0·96; p=0·0118), and extended median overall survival by 5·5 months (50·0 months, IQR 21·0 to not reached vs 44·5 months, IQR 16·5 to not reached; p=0·04). Zoledronic acid also significantly improved progression-free survival by 12% (95% CI 2-20) versus clodronic acid (HR 0·88, 95% CI 0·80-0·98; p=0·0179), and increased median progression-free survival by 2·0 months (19·5 months, IQR 9·0-38·0 vs 17·5 months, IQR 8·5-34·0; p=0·07). Rates of complete, very good partial, or partial response did not differ significantly between the zoledronic acid and clodronic acid groups for patients receiving intensive induction chemotherapy (432 patients [78%] vs 422 [76%]; p=0·43) or non-intensive induction chemotherapy (215 [50%] vs 195 [46%]; p=0·18). Both bisphosphonates were generally well tolerated, with similar occurrence of acute renal failure and treatment-emergent serious adverse events, but zoledronic acid was associated with higher rates of confirmed osteonecrosis of the jaw (35 [4%]) than was clodronic acid (3 [<1%]).
Consistent with the potential anticancer activity of zoledronic acid, overall survival improved independently of prevention of skeletal-related events, showing that zoledronic acid has treatment benefits beyond bone health. These findings support immediate treatment with zoledronic acid in patients with newly diagnosed multiple myeloma, not only for prevention of skeletal-related events, but also for potential antimyeloma benefits.
Medical Research Council (London, UK), with unrestricted educational grants from Novartis, Schering Health Care, Chugai, Pharmion, Celgene, and Ortho Biotech.
双膦酸盐可降低恶性骨病患者的骨骼事件风险,唑来膦酸在临床前和临床研究中显示出潜在的抗癌作用。我们旨在确定双膦酸盐是否会影响多发性骨髓瘤患者的临床结局。
从英国 120 个中心招募了年龄在 18 岁及以上的新诊断多发性骨髓瘤患者。通过自动电话服务,使用计算机生成的随机序列将患者平均分配到唑来膦酸组(每 3-4 周输注 4 mg)或氯膦酸组(每天口服 1600 mg)。患者还接受强化或非强化诱导化疗。没有研究人员、工作人员或患者对治疗分配进行盲法,双膦酸盐和维持治疗至少持续到疾病进展。主要终点是总生存、无进展生存和总缓解率。我们使用 Cox 比例风险模型评估无进展生存和总生存的组间差异,并使用逻辑回归模型评估总缓解率。分析是根据意向治疗进行的。这项试验在 ISRCTN68454111 注册。
2003 年 5 月至 2007 年 11 月期间共招募了 1970 名患者,其中 1960 名符合意向治疗分析的条件:唑来膦酸组 981 名(555 名接受强化化疗,426 名接受非强化化疗);氯膦酸组 979 名(556 名接受强化化疗,423 名接受非强化化疗)。治疗截止日期为 2009 年 10 月 5 日,患者在疾病进展前接受双膦酸盐治疗的中位数时间为 350 天(IQR 137-632),中位随访时间为 3.7 年(IQR 2.9-4.7)。与氯膦酸相比,唑来膦酸降低了 16%(95%CI 4-26)的死亡率(风险比[HR]0.84,95%CI 0.74-0.96;p=0.0118),并延长了 5.5 个月的中位总生存时间(50.0 个月,IQR 21.0 至未达到 vs 44.5 个月,IQR 16.5 至未达到;p=0.04)。唑来膦酸还显著改善了 12%(95%CI 2-20)的无进展生存(HR 0.88,95%CI 0.80-0.98;p=0.0179),并延长了 2.0 个月的中位无进展生存时间(19.5 个月,IQR 9.0-38.0 vs 17.5 个月,IQR 8.5-34.0;p=0.07)。接受强化诱导化疗的患者中,唑来膦酸组与氯膦酸组的完全缓解、非常好的部分缓解或部分缓解率没有显著差异(432 名患者[78%] vs 422 名[76%];p=0.43)或非强化诱导化疗(215 名[50%] vs 195 名[46%];p=0.18)。两种双膦酸盐的一般耐受性良好,急性肾衰竭和治疗相关严重不良事件的发生率相似,但唑来膦酸相关的颌骨坏死发生率(35 名[4%])明显高于氯膦酸(3 名[1%])。
与唑来膦酸的潜在抗癌活性一致,总生存的改善独立于预防骨骼相关事件,表明唑来膦酸具有除骨骼健康以外的治疗益处。这些发现支持对新诊断的多发性骨髓瘤患者立即使用唑来膦酸治疗,不仅可以预防骨骼相关事件,还可以潜在地抑制骨髓瘤。
医学研究委员会(英国伦敦),得到了诺华、先灵葆雅、日本中外制药、赛尔基因、安进和 Ortho Biotech 的无限制教育赠款。