Cancer Research UK Children's Cancer Group, School of Cancer and Enabling Sciences, University of Manchester, Manchester Academic Health Science Centre, Central Manchester University Hospitals Foundation Trust, Manchester, UK.
Lancet. 2010 Dec 11;376(9757):2009-17. doi: 10.1016/S0140-6736(10)62002-8. Epub 2010 Dec 3.
Although survival of children with acute lymphoblastic leukaemia has improved greatly in the past two decades, the outcome of those who relapse has remained static. We investigated the outcome of children with acute lymphoblastic leukaemia who relapsed on present therapeutic regimens.
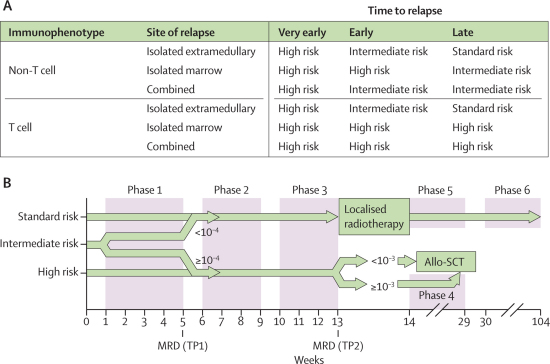
This open-label randomised trial was undertaken in 22 centres in the UK and Ireland and nine in Australia and New Zealand. Patients aged 1-18 years with first relapse of acute lymphoblastic leukaemia were stratified into high-risk, intermediate-risk, and standard-risk groups on the basis of duration of first complete remission, site of relapse, and immunophenotype. All patients were allocated to receive either idarubicin or mitoxantrone in induction by stratified concealed randomisation. Neither patients nor those giving interventions were masked. After three blocks of therapy, all high-risk group patients and those from the intermediate group with postinduction high minimal residual disease (≥10(-4) cells) received an allogenic stem-cell transplant. Standard-risk and intermediate-risk patients with postinduction low minimal residual disease (<10(-4) cells) continued chemotherapy. The primary outcome was progression-free survival and the method of analysis was intention-to-treat. Randomisation was stopped in December, 2007 because of differences in progression-free and overall survival between the two groups. This trial is registered, reference number ISCRTN45724312.
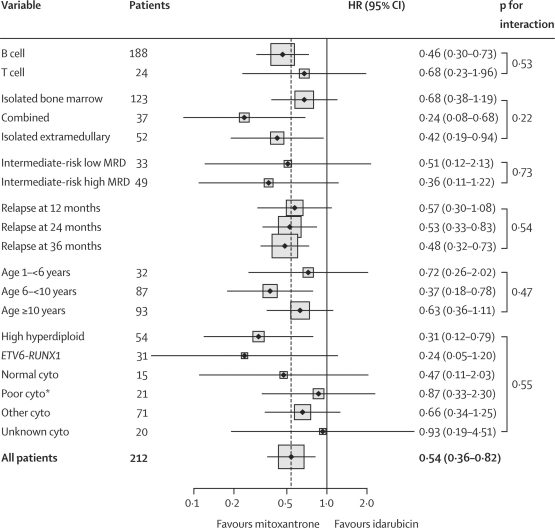
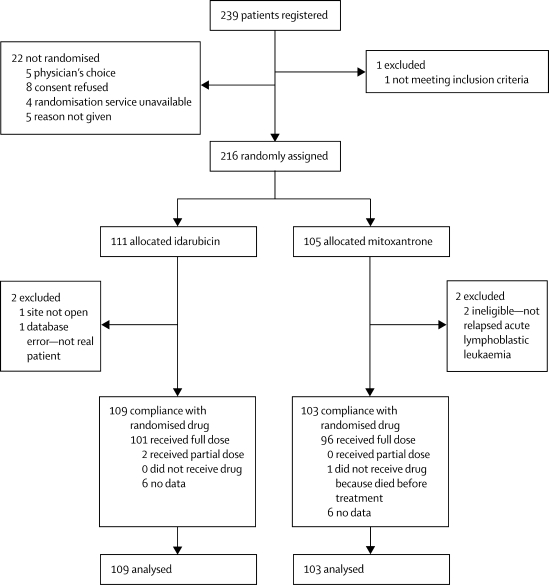
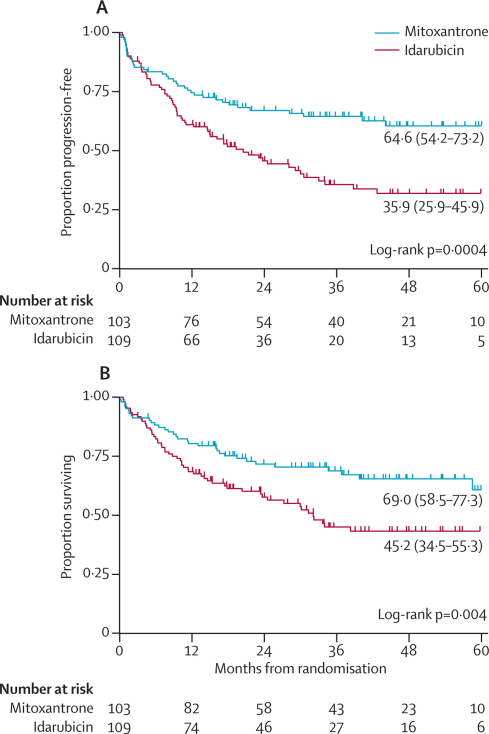
Of 239 registered patients, 216 were randomly assigned to either idarubicin (109 analysed) or mitoxantrone (103 analysed). Estimated 3-year progression-free survival was 35·9% (95% CI 25·9-45·9) in the idarubicin group versus 64·6% (54·2-73·2) in the mitoxantrone group (p=0·0004), and 3-year overall survival was 45·2% (34·5-55·3) versus 69·0% (58·5-77·3; p=0·004). Differences in progression-free survival between groups were mainly related to a decrease in disease events (progression, second relapse, disease-related deaths; HR 0·56, 0·34-0·92, p=0·007) rather than an increase in adverse treatment effects (treatment death, second malignancy; HR 0·52, 0·24-1·11, p=0·11).
As compared with idarubicin, mitoxantrone conferred a significant benefit in progression-free and overall survival in children with relapsed acute lymphobastic leukaemia, a potentially useful clinical finding that warrants further investigation.
Cancer Research UK, Leukaemia and Lymphoma Research, Cancer Council NSW, and Sporting Chance Cancer Foundation.
尽管在过去的二十年中,儿童急性淋巴细胞白血病的生存率有了很大提高,但复发患者的预后仍保持不变。我们研究了目前治疗方案下复发的儿童急性淋巴细胞白血病的预后。
这项在英国和爱尔兰的 22 个中心以及澳大利亚和新西兰的 9 个中心进行的开放标签随机试验,根据首次完全缓解的持续时间、复发部位和免疫表型,将 1-18 岁首次复发急性淋巴细胞白血病的患者分为高危、中危和标准风险组。所有患者均按分层隐匿随机化接受诱导期的伊达比星或米托蒽醌治疗。患者和干预措施提供者均不设盲。在三个疗程后,所有高危组患者和诱导后高微小残留病(≥10(-4)细胞)的中危组患者均接受同种异体干细胞移植。诱导后微小残留病低(<10(-4)细胞)的标准风险和中危风险患者继续接受化疗。主要结局是无进展生存,分析方法为意向治疗。由于两组间无进展生存和总生存的差异,随机分组于 2007 年 12 月停止。该试验已注册,注册号为 ISCRTN45724312。
在登记的 239 例患者中,216 例随机分配至伊达比星组(109 例分析)或米托蒽醌组(103 例分析)。伊达比星组估计 3 年无进展生存率为 35.9%(95%CI 25.9-45.9),米托蒽醌组为 64.6%(54.2-73.2)(p=0.0004),3 年总生存率为 45.2%(34.5-55.3)和 69.0%(58.5-77.3;p=0.004)。两组间无进展生存的差异主要与疾病事件(进展、第二次复发、疾病相关死亡)减少有关(HR 0.56,0.34-0.92,p=0.007),而不是与治疗相关不良事件(治疗死亡、第二恶性肿瘤)增加有关(HR 0.52,0.24-1.11,p=0.11)。
与伊达比星相比,米托蒽醌在复发的急性淋巴细胞白血病患儿中显著提高了无进展生存率和总生存率,这是一个潜在的有用的临床发现,值得进一步研究。
英国癌症研究中心、白血病和淋巴瘤研究中心、新南威尔士癌症委员会和体育机会癌症基金会。