Jaiswal Ashish, Shetty Ajoy P, Rajasekaran S
Department of Spine Surgery, Ganga Hospital, Coimbatore, India.
Indian J Orthop. 2007 Oct;41(4):312-7. doi: 10.4103/0019-5413.36993.
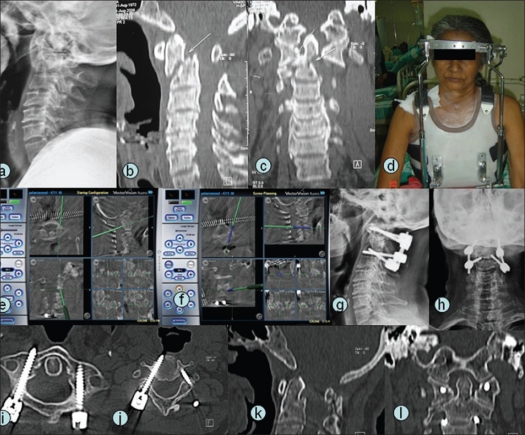
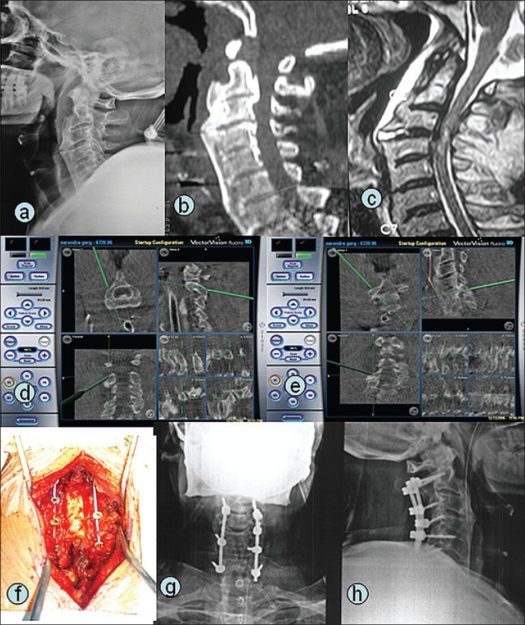
Pedicle screw fixation is the most preferred method of stabilizing unstable spinal fractures. Pedicle screw placement may be difficult in presence of fractured posterior elements, deformed spine, gross instability and spinal pathology. Challenging spine-fracture fixation is defined as the presence of one or more of the following: 1) obscured topographical landmarks as in ankylosing spondylitis, 2) fractures in occipitocervical or cervicothoracic regions and 3) preexisting altered spinal alignment. We report a series of pedicle screw insertion with guidance of navigation in difficult fixation problems..
Fourteen patients [hangman's fracture (n=3), odontoid fracture (n=4), C1C2 fracture (n=1) and spinal fracture with coexistent ankylosing spondylitis (n=6)] underwent posterior stabilization. Intraoperatively after surgical exposure, images were acquired by Iso-C 3D C-arm and transferred to navigation system. Instrumentation was performed with navigational assistance. Postoperatively, placements of pedicle screws were evaluated with radiographs and CT scan.
Sixty-seven pedicle screws (cervical, n=33; thoracic, n=6; lumbar, n=26; sacral n=2) and 15 lateral mass screws were inserted with navigation guidance. The average time of image data acquisition by Iso-C 3D C-arm and its transfer to workstation was 4 minutes (range, 2-6 minutes). Postoperative CT scan revealed ideal placement of screws in 63 pedicles (94%), grade 1 cortical breaches (<2 mm) in 3 pedicles (4.5%) and grade 2 cortical breach (2-4 mm) in one pedicle (1.5%). There were no neurovascular complications. Deep infection was encountered in one case, which settled with debridement.
Intraoperative Iso-C 3D C-arm based navigation is a useful adjunct while stabilizing challenging spinal trauma, rendering feasibility, accuracy and safety of pedicle screw placement even in difficult situations.
椎弓根螺钉固定是治疗不稳定脊柱骨折最常用的方法。在存在后部结构骨折、脊柱畸形、严重不稳定及脊柱病变的情况下,椎弓根螺钉置入可能会很困难。具有挑战性的脊柱骨折固定是指存在以下一种或多种情况:1)如强直性脊柱炎那样的局部解剖标志不清;2)枕颈或颈胸段骨折;3)既往存在脊柱排列改变。我们报告了一系列在导航引导下进行的困难固定问题中的椎弓根螺钉置入情况。
14例患者[绞刑者骨折(n = 3)、齿状突骨折(n = 4)、C1C2骨折(n = 1)及合并强直性脊柱炎的脊柱骨折(n = 6)]接受了后路稳定手术。术中手术暴露后,通过Iso-C 3D C型臂获取图像并传输至导航系统。在导航辅助下进行器械操作。术后,通过X线片和CT扫描评估椎弓根螺钉的置入情况。
在导航引导下共置入67枚椎弓根螺钉(颈椎,n = 33;胸椎,n = 6;腰椎,n = 26;骶椎,n = 2)和15枚侧块螺钉。Iso-C 3D C型臂获取图像数据并传输至工作站的平均时间为4分钟(范围2 - 6分钟)。术后CT扫描显示63枚椎弓根(94%)的螺钉置入理想,3枚椎弓根(4.5%)出现1级皮质骨破裂(<2 mm),1枚椎弓根(1.5%)出现2级皮质骨破裂(2 - 4 mm)。无神经血管并发症。1例出现深部感染,经清创后好转。
术中基于Iso-C 3D C型臂的导航在治疗具有挑战性的脊柱创伤时是一种有用的辅助手段,即使在困难情况下也能使椎弓根螺钉置入具有可行性、准确性和安全性。