Division of Nephrology and Hypertension, Department of Medicine, University of California San Diego, 200 W Arbor Drive, San Diego, CA 92103, USA.
Intensive Care Med. 2011 Feb;37(2):241-8. doi: 10.1007/s00134-010-2089-9. Epub 2010 Dec 9.
Sepsis commonly contributes to acute kidney injury (AKI); however, the frequency with which sepsis develops as a complication of AKI and the clinical consequences of this sepsis are unknown. This study examined the incidence of, and outcomes associated with, sepsis developing after AKI.
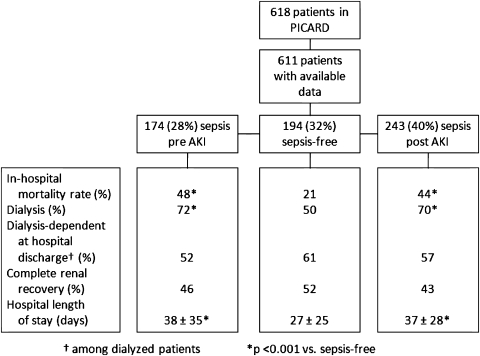
We analyzed data from 618 critically ill patients enrolled in a multicenter observational study of AKI (PICARD). Patients were stratified according to their sepsis status and timing of incident sepsis relative to AKI diagnosis.
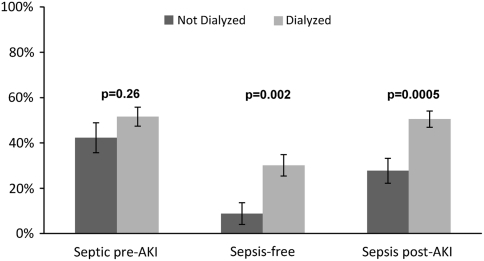
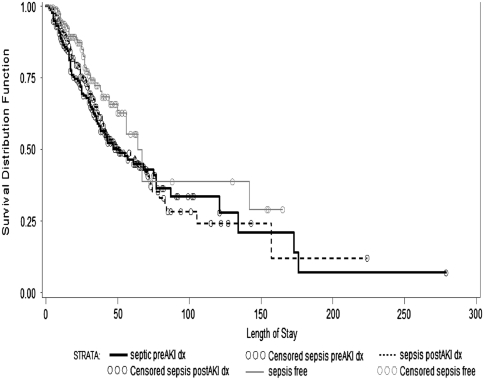
We determined the associations among sepsis, clinical characteristics, provision of dialysis, in-hospital mortality, and length of stay (LOS), comparing outcomes among patients according to their sepsis status. Among the 611 patients with data on sepsis status, 174 (28%) had sepsis before AKI, 194 (32%) remained sepsis-free, and 243 (40%) developed sepsis a median of 5 days after AKI. Mortality rates for patients with sepsis developing after AKI were higher than in sepsis-free patients (44 vs. 21%; p < 0.0001) and similar to patients with sepsis preceding AKI (48 vs. 44%; p = 0.41). Compared with sepsis-free patients, those with sepsis developing after AKI were also more likely to be dialyzed (70 vs. 50%; p < 0.001) and had longer LOS (37 vs. 27 days; p < 0.001). Oliguria, higher fluid accumulation and severity of illness scores, non-surgical procedures after AKI, and provision of dialysis were predictors of sepsis after AKI.
Sepsis frequently develops after AKI and portends a poor prognosis, with high mortality rates and relatively long LOS. Future studies should evaluate techniques to monitor for and manage this complication to improve overall prognosis.
脓毒症常导致急性肾损伤(AKI);然而,脓毒症作为 AKI 并发症的发生频率及其临床后果尚不清楚。本研究调查了 AKI 后发生脓毒症的发生率和相关结局。
我们分析了 618 例重症患者的多中心 AKI 观察研究(PICARD)的数据。患者根据其脓毒症状态和脓毒症发生与 AKI 诊断的时间进行分层。
我们确定了脓毒症与临床特征、透析的提供、院内死亡率和住院时间(LOS)之间的关联,比较了根据脓毒症状态分组的患者的结局。在有脓毒症状态数据的 611 例患者中,174 例(28%)在 AKI 之前发生脓毒症,194 例(32%)未发生脓毒症,243 例(40%)在 AKI 后中位 5 天发生脓毒症。AKI 后发生脓毒症的患者死亡率高于未发生脓毒症的患者(44% vs. 21%;p < 0.0001),与 AKI 前发生脓毒症的患者相似(48% vs. 44%;p = 0.41)。与未发生脓毒症的患者相比,AKI 后发生脓毒症的患者更有可能接受透析(70% vs. 50%;p < 0.001),且 LOS 更长(37 天 vs. 27 天;p < 0.001)。少尿、液体蓄积和疾病严重程度评分增加、AKI 后进行非手术治疗以及透析的提供是 AKI 后发生脓毒症的预测因素。
脓毒症常在 AKI 后发生,并预示预后不良,死亡率高,LOS 相对较长。未来的研究应评估监测和管理这一并发症的技术,以改善整体预后。