Department of Intensive Care Medicine, Radboud University Medical Center, HP:710, PO Box 9101, 6500, HB, Nijmegen, The Netherlands.
Department of Intensive Care and Anesthesiology, Università Cattolica Del Sacro Cuore, Largo A. Gemelli 8, 00168, Rome, Italy.
Crit Care. 2018 Aug 3;22(1):188. doi: 10.1186/s13054-018-2112-z.
Acute kidney injury (AKI) is a common complication of critical illness and is associated with worse outcomes. However, the influence of deterioration or improvement in renal function on clinical outcomes is unclear. Using a large international database, we evaluated the prevalence and evolution of AKI over a 7-day period and its effects on clinical outcomes in septic and non-septic critically ill patients worldwide.
From the 10,069 adult intensive care unit (ICU) patients in the Intensive Care Over Nations database, all those with creatinine and urine output data were included in this substudy. Patients who developed sepsis during the ICU stay (≥ 2 days after admission) were excluded. AKI was evaluated within 72 hours after admission and before discharge/death up to day 7 according to the Acute Kidney Injury Network (AKIN) criteria.
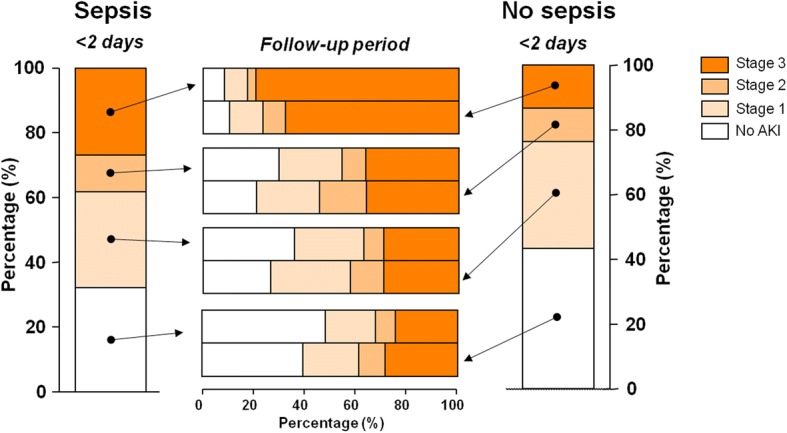
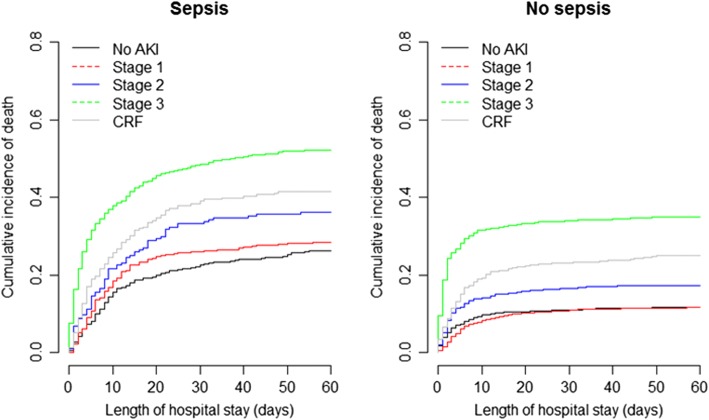
A total of 7970 patients were included, 59% of whom met AKIN criteria for AKI within the first 72 hours of the ICU stay. Twenty-four per cent of patients had sepsis on admission, of whom 68% had AKI, compared to 57% of those without sepsis on admission (p < 0.001). AKIN stage 3 (40% vs 24%, p < 0.001) and use of renal replacement therapy (20% vs 5%, p < 0.0001) were more prevalent in patients with sepsis. Patients with sepsis and AKIN stage 3 were less likely to improve to a lower stage during the 7-day follow-up period than non-septic patients with AKIN stage 3 (21% vs 32%, p < 0.0001). In-hospital mortality was related to severity of AKI and was reduced in patients in whom AKI improved compared to those who remained stable or deteriorated, but remained higher than in patients without AKI, even if there was apparent full recovery at day 7.
These findings illustrate the different kinetics of AKI in septic and non-septic ICU patients and emphasize the important impact of AKI on mortality rates even when there is apparent full renal recovery at day 7.
急性肾损伤(AKI)是危重病的常见并发症,与预后不良相关。然而,肾功能恶化或改善对临床结局的影响尚不清楚。本研究使用大型国际数据库,评估了全球脓毒症和非脓毒症危重症患者 7 天内 AKI 的患病率和演变及其对临床结局的影响。
从 Intensive Care Over Nations 数据库中纳入了 10069 名成年重症监护病房(ICU)患者,所有患者均有肌酐和尿量数据,本亚研究仅纳入了这些患者。排除在 ICU 住院期间发生脓毒症(入院后≥2 天)的患者。根据急性肾损伤网络(AKIN)标准,在入住 ICU 后 72 小时内并在出院/死亡前至第 7 天评估 AKI。
共纳入 7970 例患者,其中 59%的患者在 ICU 入住的前 72 小时内符合 AKIN 标准的 AKI。入院时 24%的患者有脓毒症,其中 68%的患者有 AKIN,而入院时无脓毒症的患者中这一比例为 57%(p<0.001)。AKIN 分期 3 级(40% vs 24%,p<0.001)和肾脏替代治疗的使用率(20% vs 5%,p<0.0001)在脓毒症患者中更为常见。与非脓毒症 AKIN 分期 3 级患者相比,脓毒症 AKIN 分期 3 级患者在 7 天随访期间更不可能改善至较低分期(21% vs 32%,p<0.0001)。院内死亡率与 AKI 的严重程度相关,与 AKI 稳定或恶化的患者相比,AKI 改善的患者死亡率降低,但仍高于无 AKI 的患者,即使在第 7 天出现明显的完全恢复。
这些发现说明了脓毒症和非脓毒症 ICU 患者 AKI 的不同动力学,并强调了 AKI 对死亡率的重要影响,即使在第 7 天出现明显的完全肾脏恢复时也是如此。