Department of Medical Physics, BC Cancer Agency-Vancouver Island Centre, Victoria, British Columbia, Canada.
Radiat Oncol. 2010 Dec 16;5:120. doi: 10.1186/1748-717X-5-120.
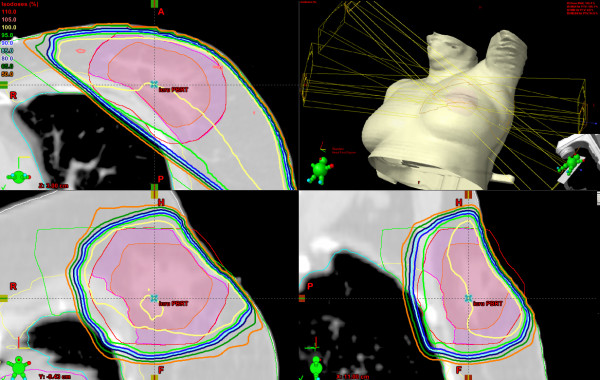
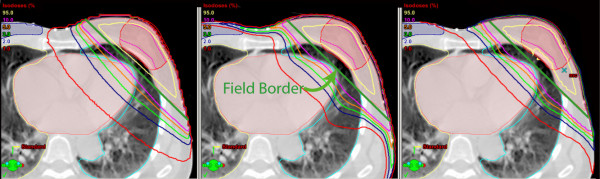
This paper compares the calculated dose to target and normal tissues when using pencil beam (PBC), superposition/convolution (AAA) and Monte Carlo (MC) algorithms for whole breast (WBI) and accelerated partial breast irradiation (APBI) treatment plans.
Plans for 10 patients who met all dosimetry constraints on a prospective APBI protocol when using PBC calculations were recomputed with AAA and MC, keeping the monitor units and beam angles fixed. Similar calculations were performed for WBI plans on the same patients. Doses to target and normal tissue volumes were tested for significance using the paired Student's t-test.
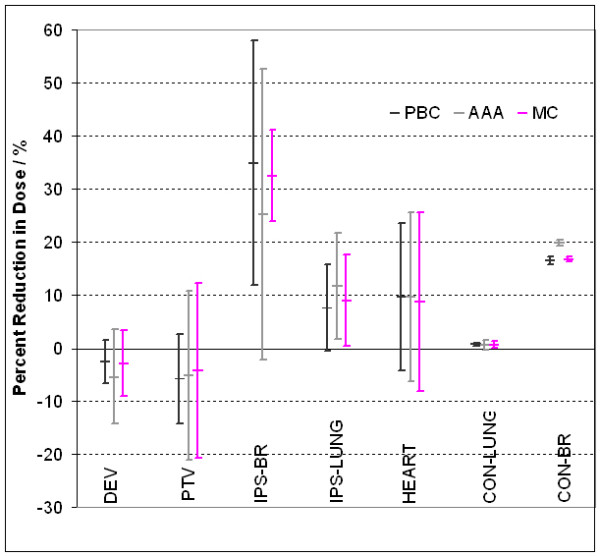
For WBI plans the average dose to target volumes when using PBC calculations was not significantly different than AAA calculations, the average PBC dose to the ipsilateral breast was 10.5% higher than the AAA calculations and the average MC dose to the ipsilateral breast was 11.8% lower than the PBC calculations. For ABPI plans there were no differences in dose to the planning target volume, ipsilateral breast, heart, ipsilateral lung, or contra-lateral lung. Although not significant, the maximum PBC dose to the contra-lateral breast was 1.9% higher than AAA and the PBC dose to the clinical target volume was 2.1% higher than AAA. When WBI technique is switched to APBI, there was significant reduction in dose to the ipsilateral breast when using PBC, a significant reduction in dose to the ipsilateral lung when using AAA, and a significant reduction in dose to the ipsilateral breast and lung and contra-lateral lung when using MC.
There is very good agreement between PBC, AAA and MC for all target and most normal tissues when treating with APBI and WBI and most of the differences in doses to target and normal tissues are not clinically significant. However, a commonly used dosimetry constraint, as recommended by the ASTRO consensus document for APBI, that no point in the contra-lateral breast volume should receive >3% of the prescribed dose needs to be relaxed to >5%.
本文比较了在全乳(WBI)和加速部分乳腺照射(APBI)治疗计划中使用笔形束(PBC)、超叠加/卷积(AAA)和蒙特卡罗(MC)算法时,靶区和正常组织的计算剂量。
对满足前瞻性 APBI 方案所有剂量学限制的 10 例患者的计划,在保持监测单位和射束角度不变的情况下,使用 AAA 和 MC 重新计算。对同一患者的 WBI 计划进行了类似的计算。使用配对学生 t 检验测试靶区和正常组织体积的剂量差异是否具有统计学意义。
对于 WBI 计划,使用 PBC 计算时靶区体积的平均剂量与 AAA 计算结果无显著差异,同侧乳腺的 PBC 平均剂量比 AAA 计算结果高 10.5%,而 MC 计算结果比 PBC 计算结果低 11.8%。对于 ABPI 计划,计划靶区、同侧乳腺、心脏、同侧肺和对侧肺的剂量无差异。尽管无统计学意义,但对侧乳腺的最大 PBC 剂量比 AAA 高 1.9%,临床靶区的 PBC 剂量比 AAA 高 2.1%。当 WBI 技术切换为 APBI 时,使用 PBC 时同侧乳腺的剂量显著降低,使用 AAA 时同侧肺的剂量显著降低,使用 MC 时同侧乳腺和肺以及对侧肺的剂量显著降低。
在使用 APBI 和 WBI 治疗时,PBC、AAA 和 MC 对所有靶区和大多数正常组织的结果非常吻合,靶区和正常组织的剂量差异大多无临床意义。然而,ASTRO 共识文件推荐的 APBI 常用剂量学限制,即对侧乳腺体积中任何一点的剂量不应超过处方剂量的 3%,需要放宽到>5%。