Division of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia School of Medicine, Charlottesville, VA 22908, USA.
J Thorac Cardiovasc Surg. 2011 Feb;141(2):543-51. doi: 10.1016/j.jtcvs.2010.10.005. Epub 2010 Dec 15.
Although consensus in cardiac surgery supports tight control of perioperative hyperglycemia (glucose<120 mg/dL), recent studies in critical care suggest moderate glycemic control may be superior. We sought to determine whether tight control or moderate glycemic control is optimal after coronary artery bypass grafting.
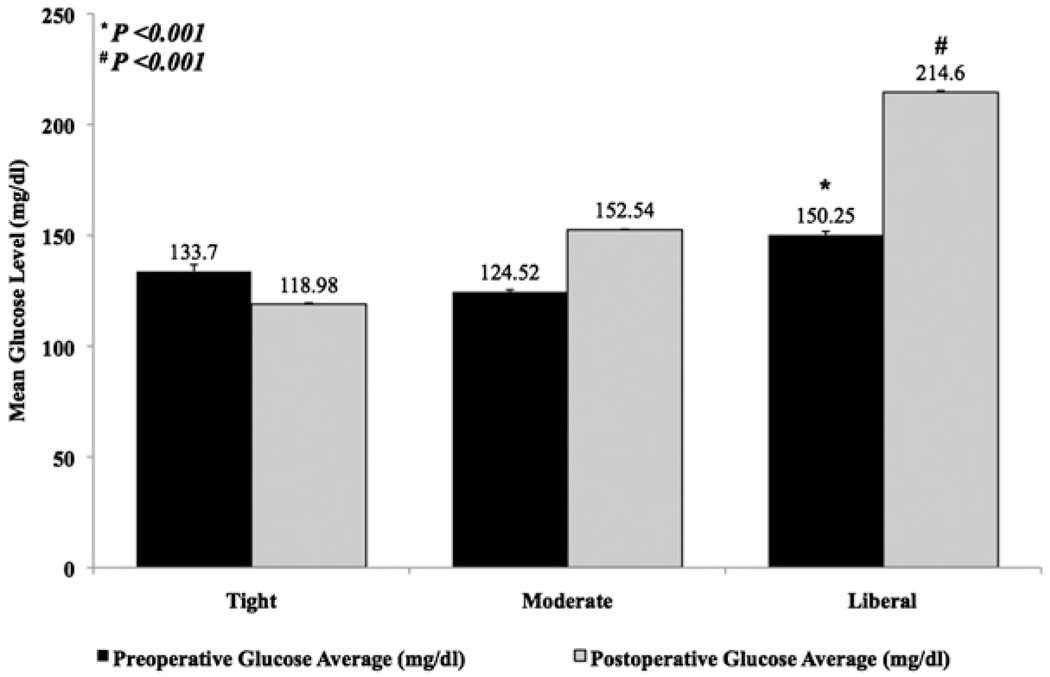
From 1995 to 2008, a total of 4658 patients with known diabetes or perioperative hyperglycemia (preoperative glycosylated hemoglobin≥8 or postoperative serum glucose>126 mg/dL) underwent isolated coronary artery bypass grafting at our institution. Patients were stratified into 3 postoperative glycemic groups: tight (≤126 mg/dL), moderate (127-179 mg/dL), and liberal (≥180 mg/dL). Preoperative risk factors, glycemic management, and postoperative outcomes were analyzed.
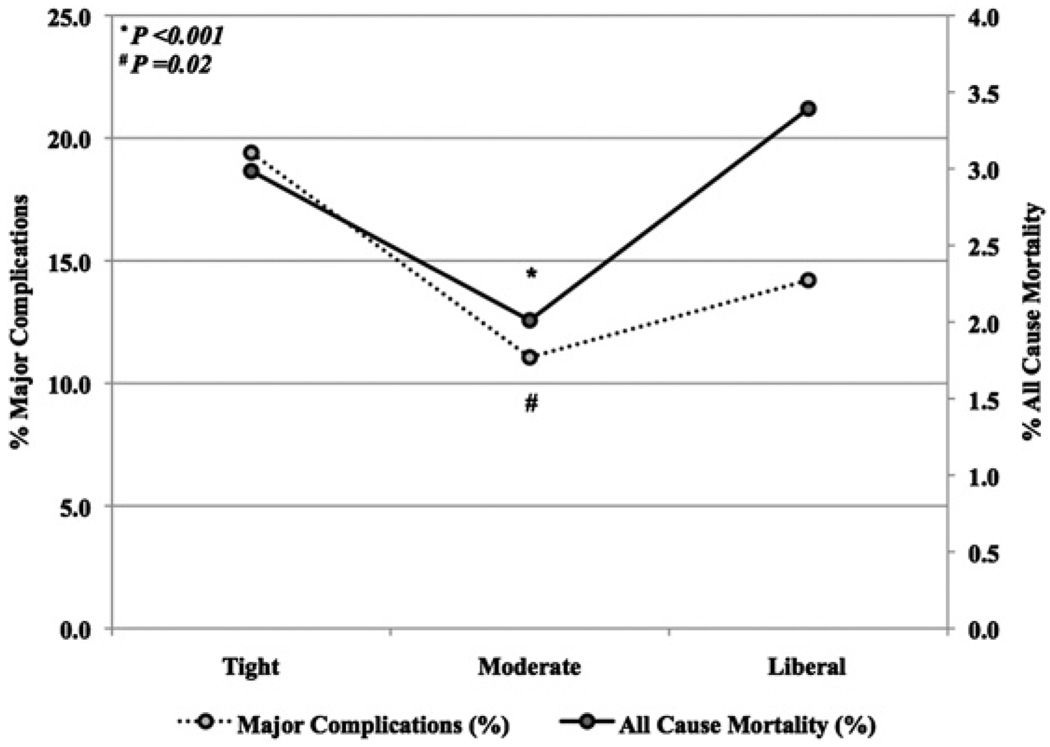
Operative mortality was 2.5% (119/4658); major complication rate was 12.5% (581/4658). Relative to moderate group, more patients in tight group had preoperative renal failure (tight 16.4%, 22/134, moderate 8.3%, 232/2785, P=.001) and underwent emergent operations (tight 5.2%, 7/134, moderate 1.9%, 52/2785, P=.007); however, Society of Thoracic Surgeons predicted mortality risk was lower in tight group (P<.001). Moderate group had lowest mortality (tight 2.9%, 4/134, moderate 2.0%, 56/2785, liberal 3.4%, 59/1739, P=.02) and incidence of major complications (tight 19.4%, 26/134, moderate 11.1%, 308/2785, liberate 14.2%, 247/1739, P<.001). Risk-adjusted major complication incidence (adjusted odds ratio 0.7, 95% confidence interval 0.58-0.87) and mortality (adjusted odds ratio 0.6, 95% confidence interval 0.37-0.83) were lower with moderate glucose control than with tight or liberal management.
Moderate glycemic control was superior to tight glycemic control, with decreased mortality and major complications, and may be ideal for patients undergoing isolated coronary artery bypass grafting.
尽管心脏外科学术界普遍支持围手术期严格控制高血糖(血糖<120mg/dL),但最近的重症监护研究表明,适度血糖控制可能更为优越。我们旨在确定在冠状动脉旁路移植术后,严格控制或适度控制血糖水平哪一种更为理想。
1995 年至 2008 年间,共有 4658 例已知糖尿病或围手术期高血糖(术前糖化血红蛋白≥8 或术后血清葡萄糖>126mg/dL)的患者在我院接受单纯冠状动脉旁路移植术。患者被分为 3 组术后血糖水平:严格控制组(≤126mg/dL)、适度控制组(127-179mg/dL)和宽松控制组(≥180mg/dL)。分析术前危险因素、血糖管理和术后结局。
手术死亡率为 2.5%(119/4658);主要并发症发生率为 12.5%(581/4658)。与中度组相比,更多的严格组患者术前有肾功能衰竭(严格组 16.4%,22/134;中度组 8.3%,232/2785,P=0.001)和急诊手术(严格组 5.2%,7/134;中度组 1.9%,52/2785,P=0.007);然而,胸外科医师协会预测死亡率在严格组较低(P<0.001)。中度组死亡率最低(严格组 2.9%,4/134;中度组 2.0%,56/2785;宽松组 3.4%,59/1739,P=0.02),主要并发症发生率最低(严格组 19.4%,26/134;中度组 11.1%,308/2785;宽松组 14.2%,247/1739,P<0.001)。调整后的主要并发症发生率(调整后优势比 0.7,95%置信区间 0.58-0.87)和死亡率(调整后优势比 0.6,95%置信区间 0.37-0.83),中度血糖控制优于严格或宽松管理。
与严格血糖控制相比,适度血糖控制可降低死亡率和主要并发症发生率,可能是单纯冠状动脉旁路移植术患者的理想选择。