From INSERM U953 Epidemiological Research Unit on Perinatal Health and Women's and Children's Health, UPMC Paris, Paris, France; and Aurore Perinatal Network, Hopital de la Croix Rousse, Hospices Civils de Lyon, Lyon 1 University, Lyon, France.
Obstet Gynecol. 2011 Jan;117(1):21-31. doi: 10.1097/AOG.0b013e318202c845.
To identify factors associated with severity of postpartum hemorrhage among characteristics of women and their delivery, the components of initial postpartum hemorrhage management, and the organizational characteristics of maternity units.
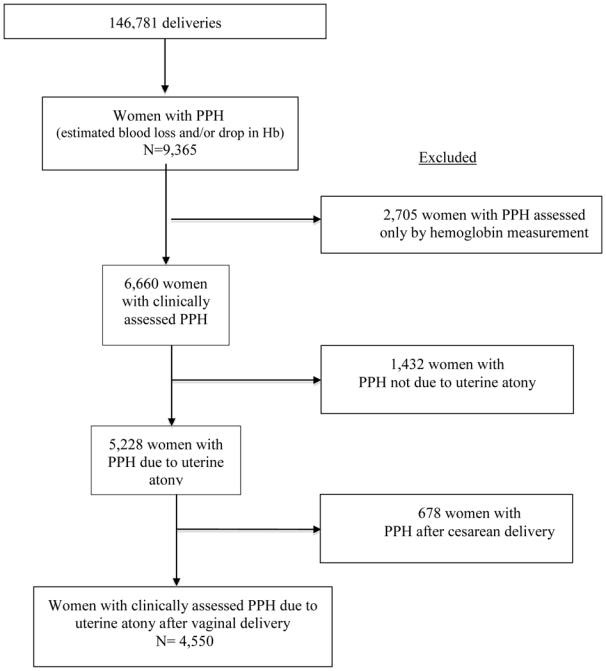
This population-based cohort study included women with postpartum hemorrhage due to uterine atony after vaginal delivery in 106 French hospitals between December 2004 and November 2006 (N=4,550). Severe postpartum hemorrhage was defined by a peripartum change in hemoglobin of 4 g/dL or more. A multivariable logistic model was used to identify factors independently associated with postpartum hemorrhage severity.
Severe postpartum hemorrhage occurred in 952 women (20.9%). In women with postpartum hemorrhage, factors independently associated with severity were: primiparity; previous postpartum hemorrhage; previous cesarean delivery; cervical ripening; prolonged labor; and episiotomy; and delay in initial care for postpartum hemorrhage. Also associated with severity was 1) administration of oxytocin more than 10 minutes after postpartum hemorrhage diagnosis: 10-20 minutes after, proportion with severe postpartum hemorrhage 24.6% compared with 20.5%, adjusted OR 1.38, 95% CI 1.03-1.85; more than 20 minutes after, 31.8% compared with 20.5%, adjusted OR 1.86, CI 1.45-2.38; 2) manual examination of the uterine cavity more than 20 minutes after (proportion with severe postpartum hemorrhage 28.2% versus 20.7%, adjusted OR 1.83, 95% CI 1.42-2.35); 3) call for additional assistance more than 10 minutes after (proportion with severe postpartum hemorrhage 29.8% versus 24.8%, adjusted OR 1.61, 95% CI 1.23-2.12 for an obstetrician, and 35.1% compared with 29.9%, adjusted OR 1.51, 95% CI 1.14-2.00 for an anesthesiologist); 4) and delivery in a public non-university hospital. Epidural analgesia was found to be a protective factor against severe blood loss in women with postpartum hemorrhage.
Aspects of labor, delivery, and their management; delay in initial care; and place of delivery are independent risk factors for severe blood loss in women with postpartum hemorrhage caused by atony.
II.
确定与产后出血严重程度相关的因素,这些因素与妇女的特征及其分娩、产后出血初始管理的组成部分以及产科单位的组织特征有关。
本基于人群的队列研究纳入了 2004 年 12 月至 2006 年 11 月期间 106 家法国医院因子宫收缩乏力导致产后出血的 4550 名阴道分娩妇女。重度产后出血定义为分娩期间血红蛋白变化 4g/dL 或以上。采用多变量逻辑模型确定与产后出血严重程度相关的独立因素。
952 名妇女(20.9%)发生重度产后出血。在产后出血妇女中,与严重程度相关的独立因素为:初产妇;既往产后出血;既往剖宫产;宫颈成熟;产程延长;会阴切开术;以及产后出血初始处理延迟。与严重程度相关的因素还包括:1)在产后出血诊断后 10 分钟以上给予催产素:诊断后 10-20 分钟,严重产后出血比例为 24.6%,调整后 OR 为 1.38,95%CI 为 1.03-1.85;20 分钟以上,严重产后出血比例为 31.8%,调整后 OR 为 1.86,95%CI 为 1.45-2.38;2)在产后出血后 20 分钟以上行宫腔检查(严重产后出血比例为 28.2%与 20.7%,调整后 OR 为 1.83,95%CI 为 1.42-2.35);3)在产后出血后 10 分钟以上呼救(严重产后出血比例为 29.8%与 24.8%,调整后 OR 为 1.61,95%CI 为 1.23-2.12,为产科医生;35.1%与 29.9%,调整后 OR 为 1.51,95%CI 为 1.14-2.00,为麻醉师);4)在公立医院分娩。硬膜外镇痛被发现是产后出血妇女严重失血的保护因素。
分娩、分娩管理以及分娩地点是产后出血妇女因宫缩乏力导致严重失血的独立危险因素。
II。