Department of Radiation Oncology, University of Pittsburgh Cancer Institute, 5230 Centre Ave, Pittsburgh, PA 15232, USA.
J Neurooncol. 2011 Aug;104(1):339-49. doi: 10.1007/s11060-010-0499-8. Epub 2010 Dec 22.
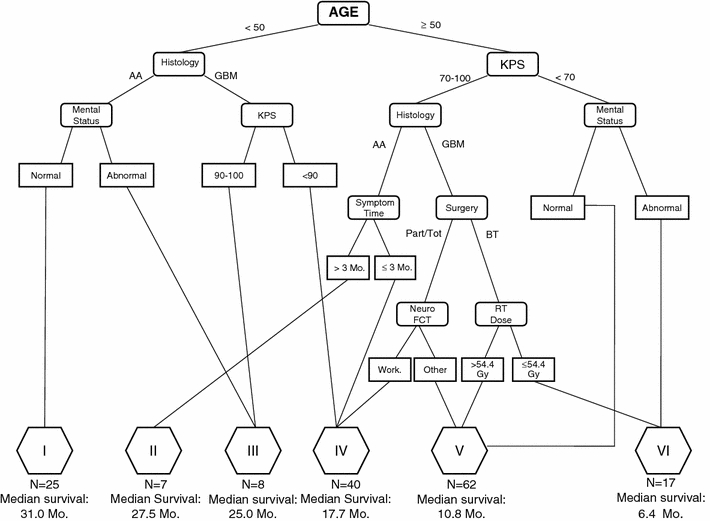
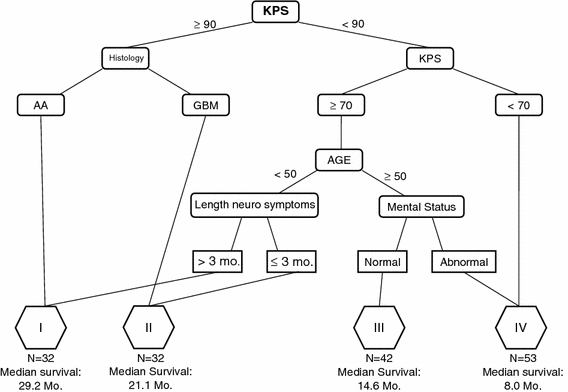
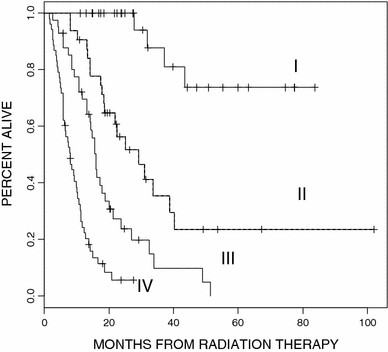
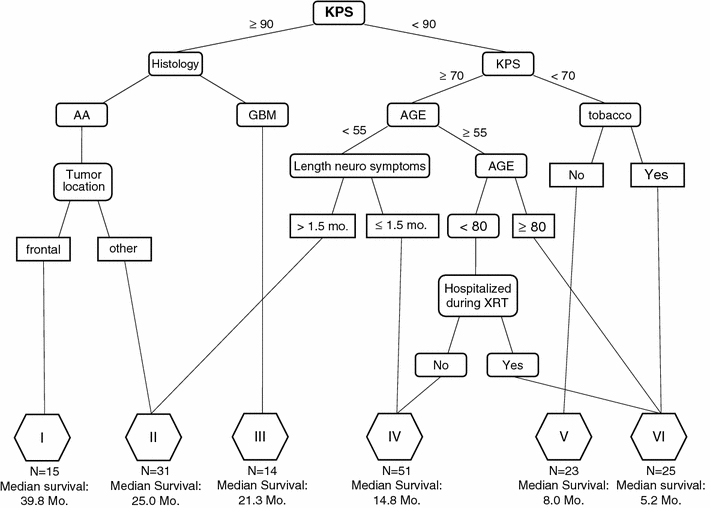
Since the development of the Radiation Therapy Oncology Group-Recursive Partitioning Analysis (RTOG-RPA) risk classes for high-grade glioma, radiation therapy in combination with temozolomide (TMZ) has become standard care. While this combination has improved survival, the prognosis remains poor in the majority of patients. Therefore, strong interest in high-grade gliomas from basic research to clinical trials persists. We sought to evaluate whether the current RTOG-RPA retains prognostic significance in the TMZ era or alternatively, if modifications better prognosticate the optimal selection of patients with similar baseline prognosis for future clinical protocols. The records of 159 patients with newly-diagnosed glioblastoma (GBM, WHO grade IV) or anaplastic astrocytoma (AA, WHO grade III) were reviewed. Patients were treated with intensity-modulated radiation therapy (IMRT) and concurrent followed by adjuvant TMZ (n = 154) or adjuvant TMZ only (n = 5). The primary endpoint was overall survival. Three separate analyses were performed: (1) application of RTOG-RPA to the study cohort and calculation of subsequent survival curves, (2) fit a new tree model with the same predictors in RTOG-RPA, and (3) fit a new tree model with an expanded predictor set. All analyses used a regression tree analysis with a survival outcome fit to formulate new risk classes. Overall median survival was 14.9 months. Using the RTOG-RPA, the six classes retained their relative prognostic significance and overall ordering, with the corresponding survival distributions significantly different from each other (P < 0.01, χ(2) statistic = 70). New recursive partitioning limited to the predictors in RTOG-RPA defined four risk groups based on Karnofsky Performance Status (KPS), histology, age, length of neurologic symptoms, and mental status. Analysis across the expanded predictors defined six risk classes, including the same five variables plus tumor location, tobacco use, and hospitalization during radiation therapy. Patients with excellent functional status, AA, and frontal lobe tumors had the best prognosis. For patients with newly-diagnosed high-grade gliomas, RTOG-RPA classes retained prognostic significance in patients treated with TMZ and IMRT. In contrast to RTOG-RPA, in our modified RPA model, KPS rather than age represented the initial split. New recursive partitioning identified potential modifications to RTOG-RPA that should be further explored with a larger data set.
自放射治疗肿瘤学组 - 递归分区分析(RTOG-RPA)高级别胶质瘤风险分类发展以来,放疗联合替莫唑胺(TMZ)已成为标准治疗方法。虽然这种联合治疗提高了生存率,但大多数患者的预后仍然较差。因此,从基础研究到临床试验,人们对高级别胶质瘤的兴趣仍然浓厚。我们试图评估当前的 RTOG-RPA 在 TMZ 时代是否仍然具有预后意义,或者是否需要修改以更好地预测具有相似基线预后的患者,以便为未来的临床方案进行最佳选择。回顾了 159 例新诊断的胶质母细胞瘤(GBM,IV 级)或间变性星形细胞瘤(AA,III 级)患者的记录。患者接受强度调制放疗(IMRT)联合同步治疗,随后接受辅助 TMZ(n=154)或单独辅助 TMZ(n=5)治疗。主要终点是总生存期。进行了三项独立分析:(1)将 RTOG-RPA 应用于研究队列并计算随后的生存曲线,(2)在 RTOG-RPA 中使用相同的预测因子拟合新的树模型,(3)使用扩展的预测因子集拟合新的树模型。所有分析均使用回归树分析和生存结果拟合来制定新的风险类别。总中位生存期为 14.9 个月。使用 RTOG-RPA,六个类别保留了相对预后意义和总体排序,相应的生存分布彼此显著不同(P<0.01,χ(2)统计量=70)。仅基于 RTOG-RPA 的预测因子进行的新递归分区定义了四个风险组,基于卡诺夫斯基表现状态(KPS)、组织学、年龄、神经症状持续时间和精神状态。在扩展预测因子的分析中定义了六个风险类别,包括相同的五个变量加上肿瘤位置、吸烟和放疗期间的住院治疗。功能状态良好、AA 和额叶肿瘤患者的预后最佳。对于新诊断的高级别胶质瘤患者,在接受 TMZ 和 IMRT 治疗的患者中,RTOG-RPA 类别保留了预后意义。与 RTOG-RPA 相反,在我们修改后的 RPA 模型中,KPS 而不是年龄代表了初始分裂。新的递归分区确定了对 RTOG-RPA 的潜在修改,需要使用更大的数据集进一步探索。