Zhou Peng, Yang Xinchun, Li Cuilan, Gao Ying, Hu Dayi
Heart Center, Beijing Chaoyang Hospital Affiliated Capital Medical University, Beijing, PRC, China.
J Cardiovasc Dis Res. 2010 Jan;1(1):12-8. doi: 10.4103/0975-3583.59979.
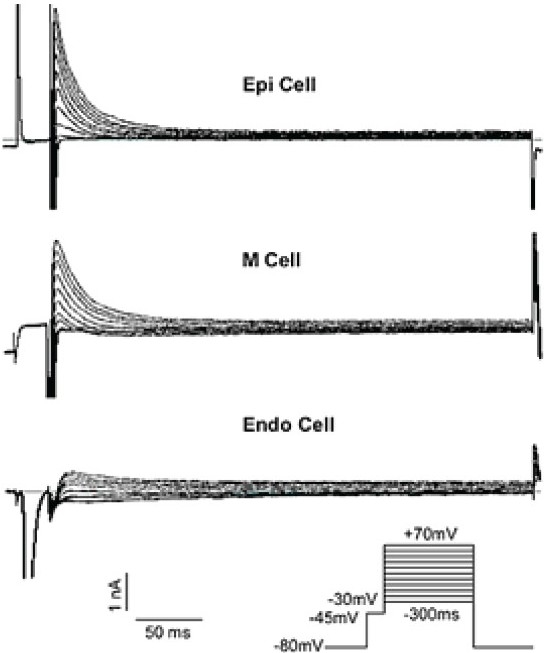
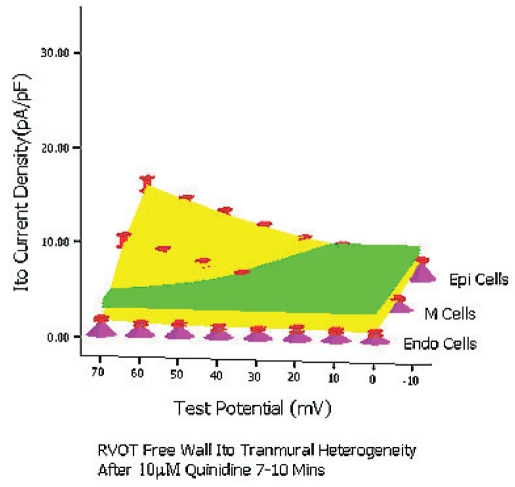
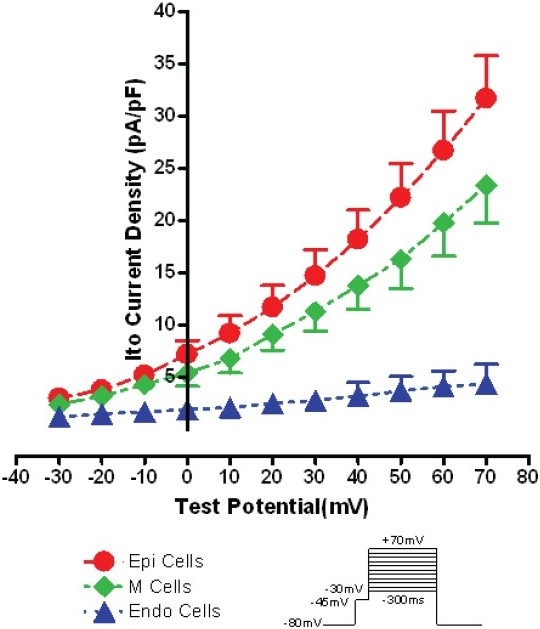
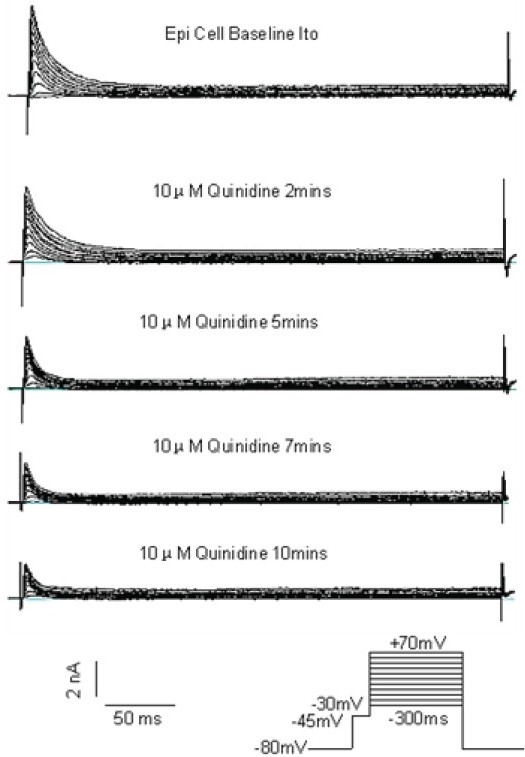
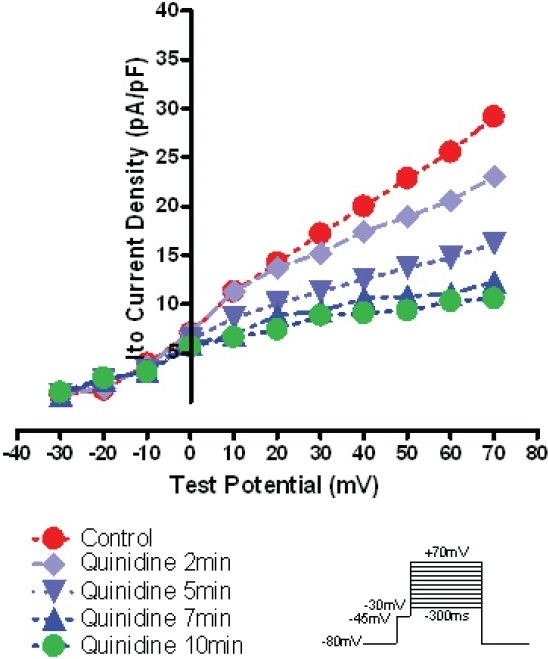
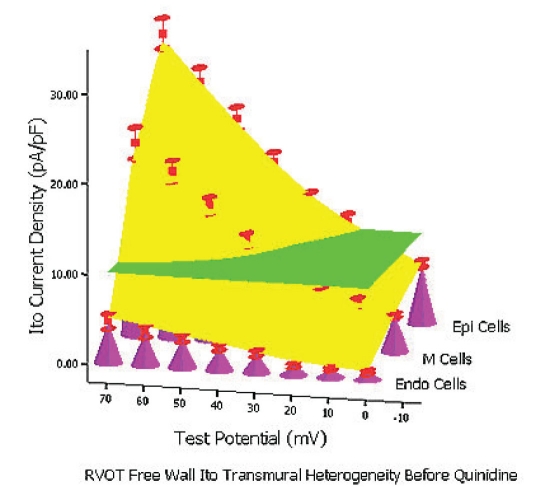
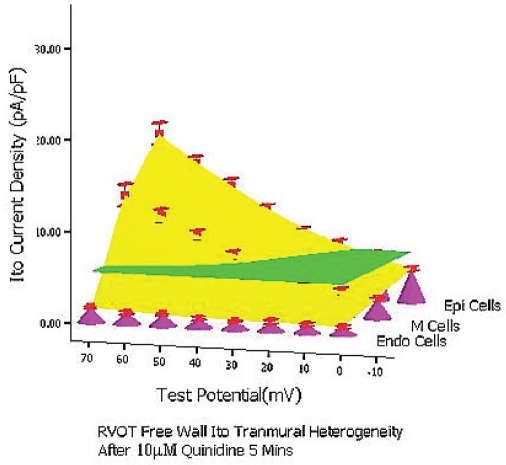
BACKGROUND#ENTITYSTARTX02014;: Electrical heterogeneity of the right ventricular outflow tract (RVOT) is regarded as one of the main electrophysiological substrates for Brugada syndrome. Recently quinidine has shown efficacy in patients with Brugada syndrome due to its ability to inhibit potassium current especially 4-aminopyridine-sensitive, non-Ca(2+) -dependent transient outward potassium current (Ito). However, much less is known on how extent quinidine in clinical therapeutic concentration range can inhibit this kind of electrical heterogeneity of RVOT Ito. METHODS AND RESULTS#ENTITYSTARTX02014;: Single RVOT free wall epicardial (Epi) cell, midmyocardial (M) cell and endocarcial (Endo) cells were used for whole-cell voltage clamping and Ito was recorded at 37°C, 0.2 Hz depolarization pulse. Evident Ito tranmural heterogeneity existed in RVOT free wall. Under the condition of baseline, of 10 μM quinidine perfusion 5 minutes (mins), and of 10 μM quinidine perfusion 7-10 mins, from 0 mV to 70 mV the whole transmural average Ito values of RVOT free wall were 10.2 pA/pF, 5.5 pA/pF and 3.5 pA/pF, respectively (between groups, P< 0.01). The inhibitory percentage of 10 μM quinidine at 5 mins and 7-10 mins steady-state level on the the whole Ito transmural heterogeneity of RVOT free wall were 46.3%±6% and 66.5%±11%, respectively. CONCLUSIONS#ENTITYSTARTX02014;: There exists a robust Ito transmural electrical heterogeneity in RVOT free wall and quinidine in clinical therapeutic concentration can depress this kind of heterogeneity effectively.
右心室流出道(RVOT)的电不均一性被认为是Brugada综合征的主要电生理基础之一。近来,奎尼丁因其抑制钾电流尤其是4-氨基吡啶敏感的、非Ca(2+)依赖性瞬时外向钾电流(Ito)的能力,在Brugada综合征患者中显示出疗效。然而,关于临床治疗浓度范围内的奎尼丁能在多大程度上抑制RVOT Ito的这种电不均一性,所知甚少。
采用单个RVOT游离壁心外膜(Epi)细胞、中层心肌(M)细胞和心内膜(Endo)细胞进行全细胞膜片钳记录,在37°C、0.2 Hz去极化脉冲下记录Ito。RVOT游离壁存在明显的Ito跨壁不均一性。在基线条件下、10 μM奎尼丁灌注5分钟以及10 μM奎尼丁灌注7 - 10分钟时,从0 mV至70 mV,RVOT游离壁的全跨壁平均Ito值分别为10.2 pA/pF、5.5 pA/pF和3.5 pA/pF(组间比较,P<0.01)。10 μM奎尼丁在5分钟和7 - 10分钟稳态水平时对RVOT游离壁Ito全跨壁不均一性的抑制率分别为46.3%±6%和66.5%±11%。
RVOT游离壁存在显著的Ito跨壁电不均一性,临床治疗浓度的奎尼丁可有效降低这种不均一性。