Choi Se Hyun, Kim Hyun Jung
Department of Pediatrics, College of Medicine, Eulji University, Daejeon, Korea.
Korean J Pediatr. 2010 Sep;53(9):855-8. doi: 10.3345/kjp.2010.53.9.855. Epub 2010 Sep 13.
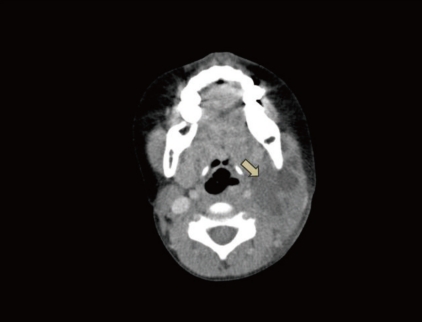
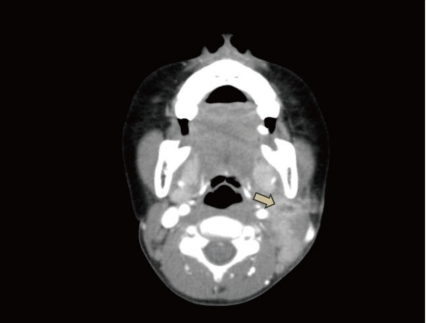
Kawasaki disease (KD) causes multisystemic vasculitis but infrequently manifests with deep neck infections, such as a peritonsillar abscess, peritonsillar or deep neck cellulitis, suppurative parapharyngeal infection, or retropharyngeal abscess. As its etiology is still unknown, the diagnosis is usually made based on typical symptoms. The differential diagnosis between KD and deep neck infections is important, considering the variable head and neck manifestations of KD. There are several reports on KD patients who were initially diagnosed with retropharyngeal abscess on on computed tomography scans (CT). However, the previously reported cases did not have abscess or fluid collection on retropharyngeal aspiration. Therefore, false-positive neck CT scans have been obtained, until recently. In this case, suspected neck abscess in patients with KD unresponsive to intravenous immunoglobulin could signal the possible coexistence of suppurative cervical lymphadenitis.
川崎病(KD)可导致多系统血管炎,但很少表现为深部颈部感染,如扁桃体周围脓肿、扁桃体周围或深部颈部蜂窝织炎、化脓性咽旁感染或咽后脓肿。由于其病因尚不清楚,诊断通常基于典型症状。鉴于KD在头颈部的表现多样,KD与深部颈部感染的鉴别诊断很重要。有几篇关于KD患者的报道,这些患者最初在计算机断层扫描(CT)上被诊断为咽后脓肿。然而,之前报道的病例在咽后穿刺抽吸时并未发现脓肿或积液。因此,直到最近,颈部CT扫描出现了假阳性结果。在这种情况下,对静脉注射免疫球蛋白无反应的KD患者出现疑似颈部脓肿,可能预示着化脓性颈淋巴结炎的并存。