Laboratory of Kidney Toxicology and Regeneration, Renal Division, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Harvard Institutes of Medicine, Boston, MA, USA.
Wiley Interdiscip Rev Syst Biol Med. 2011 Sep-Oct;3(5):606-18. doi: 10.1002/wsbm.133. Epub 2010 Dec 31.
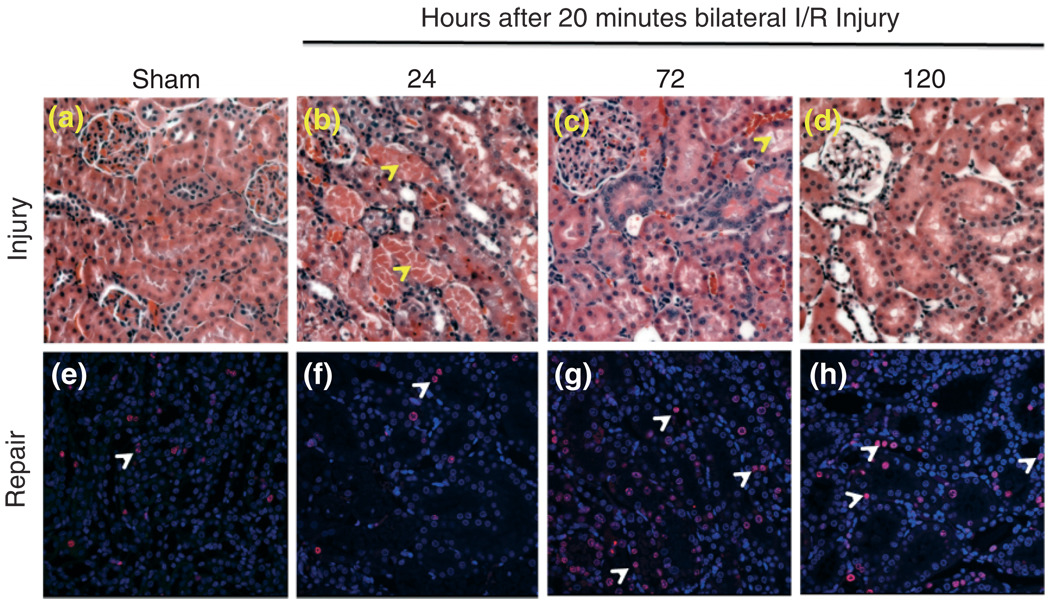
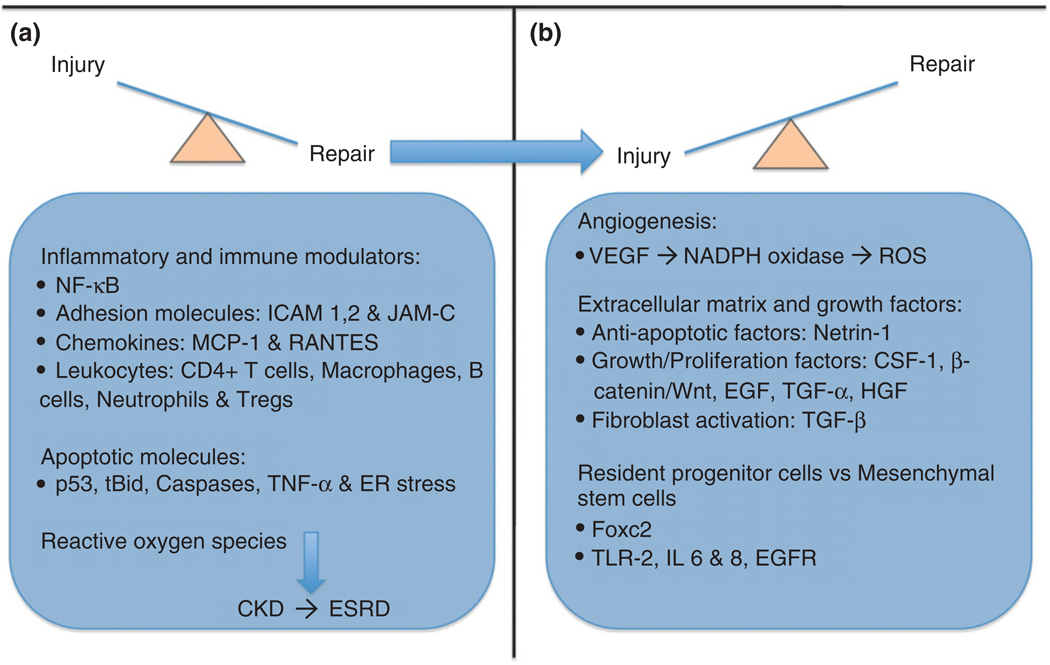
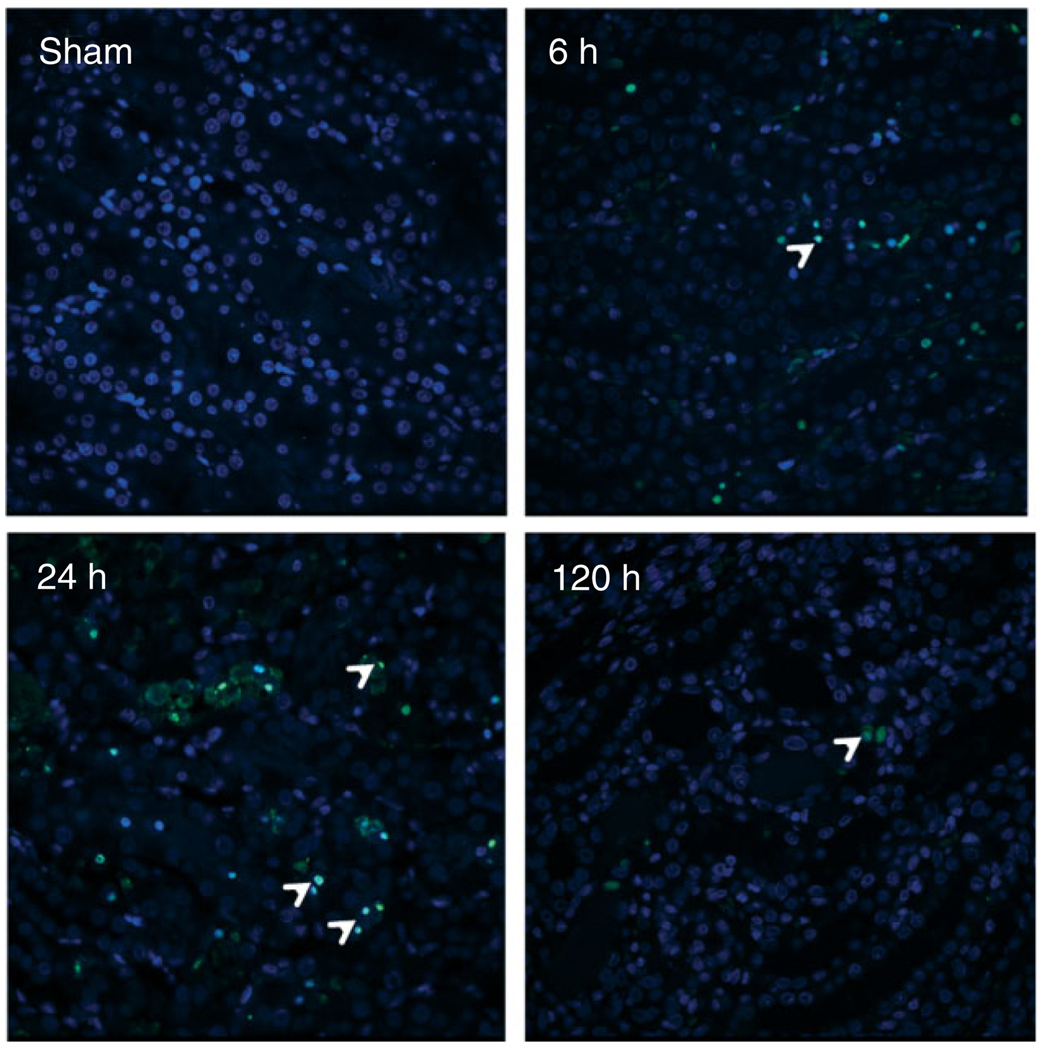
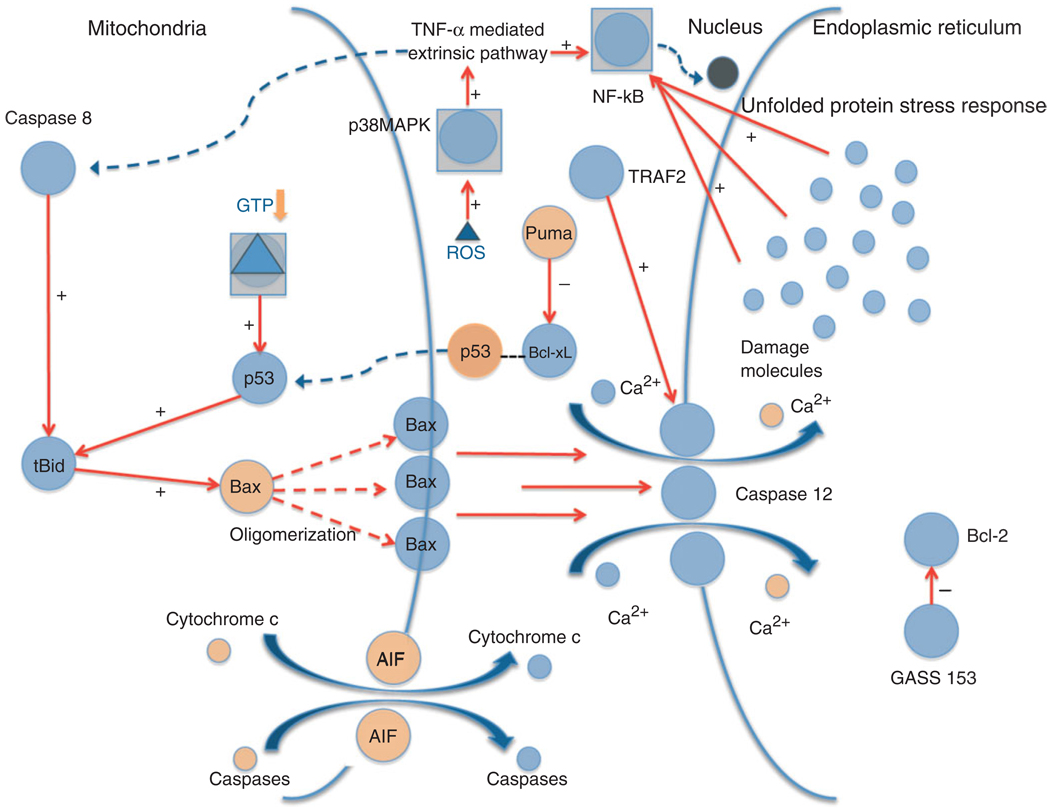
Acute kidney injury (AKI) may result from ischemia or by the use of nephrotoxic agents. The incidence of AKI is variable, depends on comorbidities, and ranges from 5 to 35% in all hospitalized patients. The mechanisms of kidney injury exist within a large network of signaling pathways driven by interplay of inflammatory cytokines/chemokines, reactive oxygen species (ROS), and apoptotic factors. The effects and progression of injury overlap extensively with the remarkable ability of the kidney to repair itself both by intrinsic and extrinsic mechanisms that involve specific cell receptors/ligands as well as possible paracrine influences. The fact that kidney injury is usually part of a generalized comorbid condition makes it all the more challenging in terms of assessment of severity. In this review, we attempt to analyze the mechanisms of ischemic injury and repair in acute and chronic kidney disease from the perspectives of both preclinical and human studies.
急性肾损伤(AKI)可能由缺血或使用肾毒性药物引起。AKI 的发病率是可变的,取决于合并症,在所有住院患者中的范围为 5%至 35%。肾损伤的机制存在于由炎症细胞因子/趋化因子、活性氧(ROS)和凋亡因子相互作用驱动的大型信号通路网络中。损伤的影响和进展与肾脏通过内在和外在机制自身修复的显著能力广泛重叠,这些机制涉及特定的细胞受体/配体以及可能的旁分泌影响。事实上,肾损伤通常是全身性合并症的一部分,这使得评估其严重程度更加具有挑战性。在这篇综述中,我们试图从临床前和人体研究的角度分析急性和慢性肾脏病中缺血性损伤和修复的机制。