Medical Research Council Laboratories, Banjul, The Gambia.
Malar J. 2011 Jan 7;10:2. doi: 10.1186/1475-2875-10-2.
Individual malaria interventions provide only partial protection in most epidemiological situations. Thus, there is a need to investigate whether combining interventions provides added benefit in reducing mortality and morbidity from malaria. The potential benefits of combining IPT in children (IPTc) with home management of malaria (HMM) was investigated.
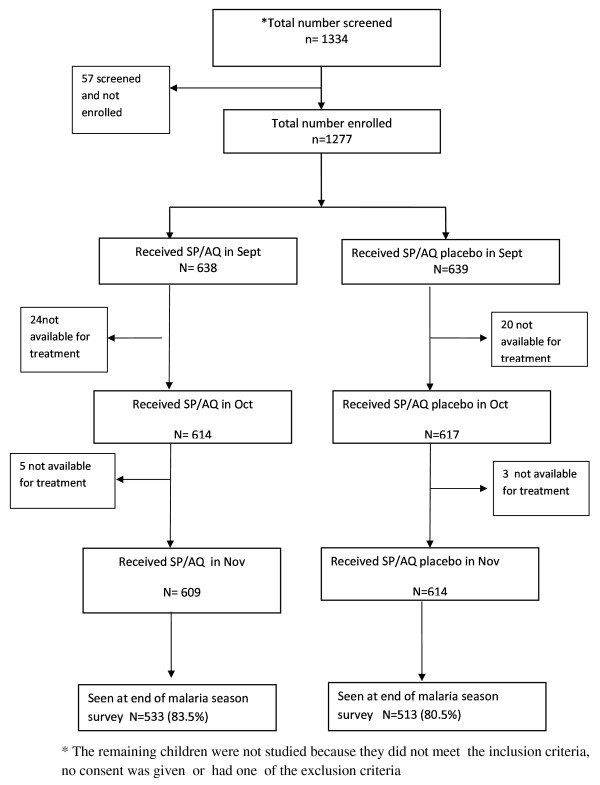
During the 2008 malaria transmission season, 1,277 children under five years of age resident in villages within the rural Farafenni demographic surveillance system (DSS) in North Bank Region, The Gambia were randomized to receive monthly IPTc with a single dose of sulphadoxine/pyrimethamine (SP) plus three doses of amodiaquine (AQ) or SP and AQ placebos given by village health workers (VHWs) on three occasions during the months of September, October and November, in a double-blind trial. Children in all study villages who developed an acute febrile illness suggestive of malaria were treated by VHWs who had been taught how to manage malaria with artemether-lumefantrine (Coartem™). The primary aims of the project were to determine whether IPTc added significant benefit to HMM and whether VHWs could effectively combine the delivery of both interventions.
The incidence of clinical attacks of malaria was very low in both study groups. The incidence rate of malaria in children who received IPTc was 0.44 clinical attacks per 1,000 child months at risk while that for control children was 1.32 per 1,000 child months at risk, a protective efficacy of 66% (95% CI -23% to 96%; p = 0.35). The mean (standard deviation) haemoglobin concentration at the end of the malaria transmission season was similar in the two treatment groups: 10.2 (1.6) g/dL in the IPTc group compared to 10.3 (1.5) g/dL in the placebo group. Coverage with IPTc was high, with 94% of children receiving all three treatments during the study period.
Due to the very low incidence of malaria, no firm conclusion can be drawn on the added benefit of IPTc in preventing clinical episodes of malaria among children who had access to HMM in The Gambia. However, the study showed that VHWs can successfully combine provision of HMM with provision of IPTc.
在大多数流行病学情况下,单一的疟疾干预措施只能提供部分保护。因此,需要研究是否结合干预措施可以在降低疟疾死亡率和发病率方面提供额外的益处。研究了在儿童中联合使用间歇性预防治疗(IPT)和家庭疟疾管理(HMM)的潜在益处。
在 2008 年疟疾传播季节期间,居住在冈比亚北岸区法尔范尼农村人口监测系统(DSS)内村庄的 1,277 名五岁以下儿童被随机分配接受每月一次的 IPTc,给予一剂磺胺多辛/乙胺嘧啶(SP)加三剂阿莫地喹(AQ),或由乡村卫生工作者(VHWs)在 9 月、10 月和 11 月的三个月内三次给予 SP 和 AQ 安慰剂,这是一项双盲试验。所有研究村庄中出现疑似疟疾的急性发热性疾病的儿童均由接受过用青蒿素-哌喹(Coartem™)治疗疟疾培训的 VHWs 治疗。该项目的主要目的是确定 IPTc 是否对 HMM 有显著益处,以及 VHWs 是否能够有效地结合两种干预措施的实施。
在两个研究组中,临床疟疾发作的发生率都非常低。接受 IPTc 的儿童的疟疾发病率为每 1,000 名儿童月风险 0.44 例临床攻击,而对照组儿童的发病率为每 1,000 名儿童月风险 1.32 例,保护效力为 66%(95%CI-23%至 96%;p=0.35)。疟疾传播季节结束时,两组的平均(标准差)血红蛋白浓度相似:IPTc 组为 10.2(1.6)g/dL,安慰剂组为 10.3(1.5)g/dL。IPTc 的覆盖率很高,94%的儿童在研究期间接受了所有三次治疗。
由于疟疾的发病率非常低,因此无法确定在冈比亚获得 HMM 的儿童中,IPTc 预防临床疟疾发作的额外益处。然而,该研究表明,VHWs 可以成功地将 HMM 的提供与 IPTc 的提供相结合。