Department of Intensive Care Medicine and Laboratory of Experimental Intensive Care and Anesthesiology, Academic Medical Center, Meibergdreef 9, Amsterdam NL-1105 AZ, The Netherlands.
Crit Care. 2011;15(1):R59. doi: 10.1186/cc10032. Epub 2011 Feb 11.
Blood transfusion is associated with increased morbidity and mortality in cardiac surgery patients, but cause-and-effect relations remain unknown. We hypothesized that blood transfusion is associated with changes in pulmonary and systemic inflammation and coagulation occurring in patients who do not meet the clinical diagnosis of transfusion-related acute lung injury (TRALI).
We performed a case control study in a mixed medical-surgical intensive care unit of a university hospital in the Netherlands. Cardiac surgery patients (n = 45) were grouped as follows: those who received no transfusion, those who received a restrictive transfusion (one two units of blood) or those who received multiple transfusions (at least five units of blood). Nondirected bronchoalveolar lavage fluid (BALF) and blood were obtained within 3 hours postoperatively. Normal distributed data were analyzed using analysis of variance and Dunnett's post hoc test. Nonparametric data were analyzed using the Kruskal-Wallis and Mann-Whitney U tests.
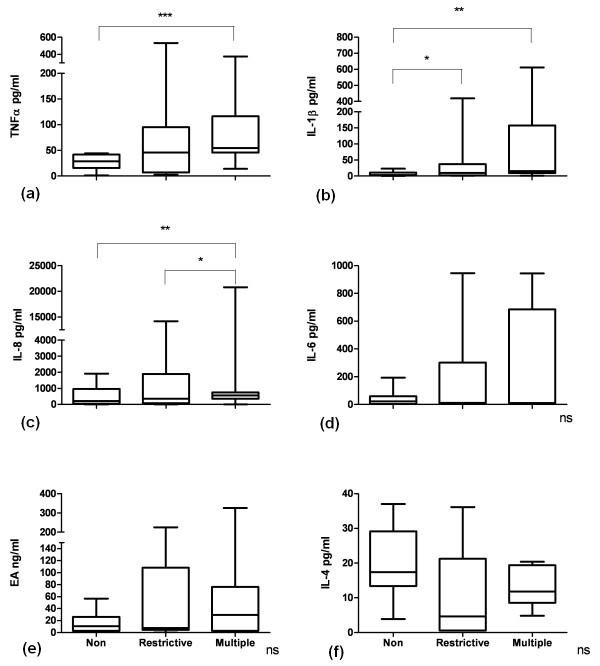
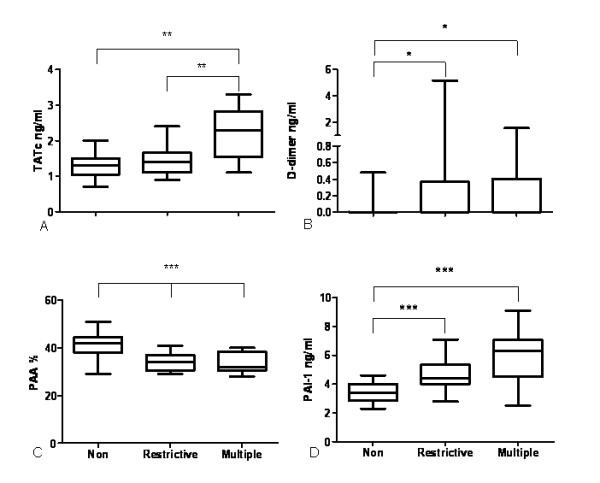
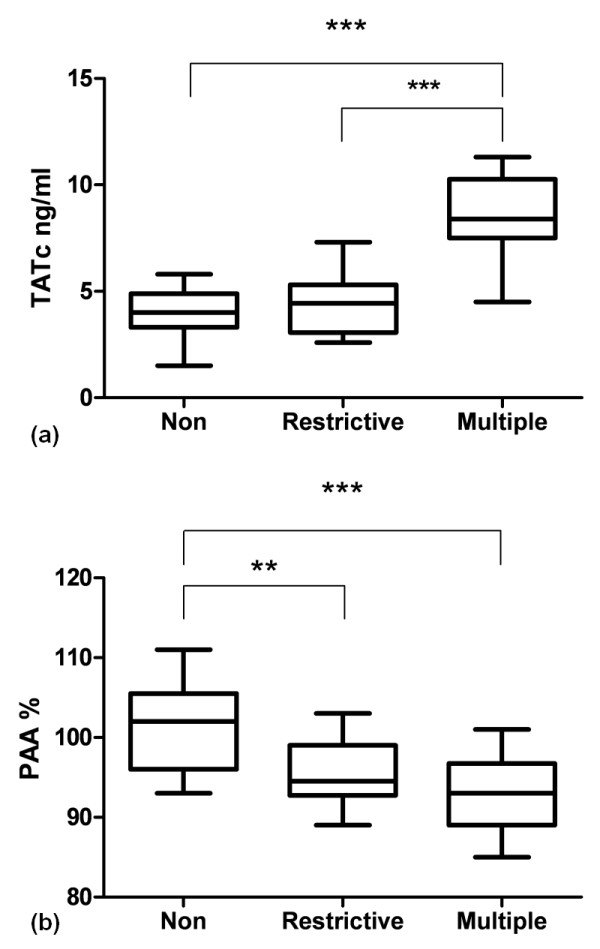
Restrictive transfusion increased BALF levels of interleukin (IL)-1β and D-dimer compared to nontransfused controls (P < 0.05 for all), and IL-1β levels were further enhanced by multiple transfusions (P < 0.01). BALF levels of IL-8, tumor necrosis factor α (TNFα) and thrombin-antithrombin complex (TATc) were increased after multiple transfusions (P < 0.01, P < 0.001 and P < 0.01, respectively) compared to nontransfused controls, but not after restrictive transfusions. Restrictive transfusions were associated with increased pulmonary levels of plasminogen activator inhibitor 1 compared to nontransfused controls with a further increase after multiple transfusions (P < 0.001). Concomitantly, levels of plasminogen activator activity (PAA%) were lower (P < 0.001), indicating impaired fibrinolysis. In the systemic compartment, transfusion was associated with a significant increase in levels of TNFα, TATc and PAA% (P < 0.05).
Transfusion during cardiac surgery is associated with activation of inflammation and coagulation in the pulmonary compartment of patients who do not meet TRALI criteria, an effect that was partly dose-dependent, suggesting transfusion as a mediator of acute lung injury. These pulmonary changes were accompanied by systemic derangement of coagulation.
输血与心脏手术患者的发病率和死亡率增加有关,但因果关系尚不清楚。我们假设输血与未达到输血相关急性肺损伤(TRALI)临床诊断的患者发生的肺部和全身炎症及凝血变化有关。
我们在荷兰一所大学医院的混合内科-外科重症监护病房进行了病例对照研究。心脏手术患者(n=45)分为以下几组:未输血组、限制性输血组(输 2 个单位血)和多次输血组(至少输 5 个单位血)。术后 3 小时内采集非定向支气管肺泡灌洗液(BALF)和血液。正态分布数据采用方差分析和 Dunnett 事后检验进行分析。非参数数据采用 Kruskal-Wallis 和 Mann-Whitney U 检验进行分析。
与未输血的对照组相比,限制性输血增加了 BALF 中白细胞介素(IL)-1β和 D-二聚体的水平(所有 P 值均<0.05),多次输血进一步增加了 IL-1β的水平(P<0.01)。与未输血的对照组相比,多次输血后 BALF 中白细胞介素-8、肿瘤坏死因子-α(TNFα)和凝血酶-抗凝血酶复合物(TATc)的水平升高(分别为 P<0.01、P<0.001 和 P<0.01),但限制性输血后未见升高。与未输血的对照组相比,限制性输血后肺组织中纤溶酶原激活物抑制剂 1 的水平升高,多次输血后进一步升高(P<0.001)。同时,纤溶酶原激活物活性(PAA%)降低(P<0.001),表明纤溶功能受损。在全身方面,输血与 TNFα、TATc 和 PAA%水平的显著升高有关(P<0.05)。
心脏手术期间输血与未达到 TRALI 标准的患者肺部炎症和凝血激活有关,这种作用部分呈剂量依赖性,提示输血是急性肺损伤的一个介导因素。这些肺部变化伴随着全身凝血系统的紊乱。