Department of Anaesthesiology and Intensive Care Medicine, University Hospital Schleswig-Holstein, Campus Kiel, Schwanenweg 21, Kiel 24105, Germany.
Crit Care. 2011;15(1):R61. doi: 10.1186/cc10035. Epub 2011 Feb 14.
Mild therapeutic hypothermia (MTH) has been shown to result in better neurological outcome after cardiopulmonary resuscitation. Percutaneous coronary intervention (PCI) may also be beneficial in patients after out-of-hospital cardiac arrest (OHCA).
A selected cohort study of 2,973 prospectively documented adult OHCA patients within the German Resuscitation Registry between 2004 and 2010. Data were analyzed by backwards stepwise binary logistic regression to identify the impact of MTH and PCI on both 24-hour survival and neurological outcome that was based on cerebral performance category (CPC) at hospital discharge. Odds ratios (95% confidence intervals) were calculated adjusted for the following confounding factors: age, location of cardiac arrest, presumed etiology, bystander cardiopulmonary resuscitation, witnessing, first electrocardiogram rhythm, and thrombolysis.
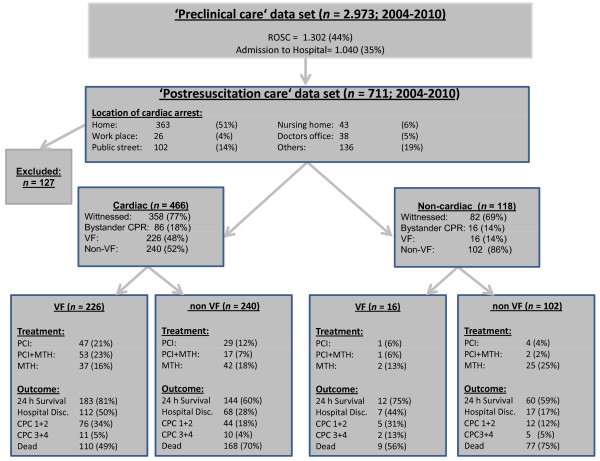
The Preclinical care dataset included 2,973 OHCA patients with 44% initial return of spontaneous circulation (n = 1,302) and 35% hospital admissions (n = 1,040). Seven hundred and eleven out of these 1,040 OHCA patients (68%) were also registered within the Postresuscitation care dataset. Checking for completeness of datasets required the exclusion of 127 Postresuscitation care cases, leaving 584 patients with complete data for final analysis. In patients without PCI (n = 430), MTH was associated with increased 24-hour survival (8.24 (4.24 to 16.0), P < 0.001) and the proportion of patients with CPC 1 or CPC 2 at hospital discharge (2.13 (1.17 to 3.90), P < 0.05) as an independent factor. In normothermic patients (n = 405), PCI was independently associated with increased 24-hour survival (4.46 (2.26 to 8.81), P < 0.001) and CPC 1 or CPC 2 (10.81 (5.86 to 19.93), P < 0.001). Additional analysis of all patients (n = 584) revealed that 24-hour survival was increased by MTH (7.50 (4.12 to 13.65), P < 0.001) and PCI (3.88 (2.11 to 7.13), P < 0.001), while the proportion of patients with CPC 1 or CPC 2 was significantly increased by PCI (5.66 (3.54 to 9.03), P < 0.001) but not by MTH (1.27 (0.79 to 2.03), P = 0.33), although an unadjusted Fisher exact test suggested a significant effect of MTH (unadjusted odds ratio 1.83 (1.23 to 2.74), P < 0.05).
PCI may be an independent predictor for good neurological outcome (CPC 1 or CPC 2) at hospital discharge. MTH was associated with better neurological outcome, although subsequent logistic regression analysis did not show statistical significance for MTH as an independent predictor for good neurological outcome. Thus, postresuscitation care on the basis of standardized protocols including coronary intervention and hypothermia may be beneficial after successful resuscitation. One of the main limitations may be a selection bias for patients subjected to PCI and MTH.
研究表明,心肺复苏后轻度治疗性低体温(MTH)可导致更好的神经功能恢复。经皮冠状动脉介入治疗(PCI)也可能对院外心脏骤停(OHCA)患者有益。
这是一项在德国复苏登记处(2004 年至 2010 年)进行的前瞻性、有 2973 例成年 OHCA 患者的队列研究。通过向后逐步二元逻辑回归分析,识别 MTH 和 PCI 对 24 小时生存率和神经功能的影响,后者基于出院时的脑功能分类(CPC)。计算了调整以下混杂因素后的优势比(95%置信区间):年龄、心脏骤停位置、假定病因、旁观者心肺复苏、目击者、首次心电图节律和溶栓。
在临床前护理数据集中,包括 2973 例 OHCA 患者,44%初始自发循环恢复(n=1302)和 35%住院(n=1040)。在这些 1040 例 OHCA 患者中,有 711 例(68%)也在复苏后护理数据集中注册。为了检查数据集的完整性,需要排除复苏后护理数据集的 127 例病例,最终有 584 例完整数据的患者可用于最终分析。在未行 PCI 的患者(n=430)中,MTH 与 24 小时生存率增加(8.24(4.24 至 16.0),P<0.001)和出院时 CPC 1 或 CPC 2 患者比例增加(2.13(1.17 至 3.90),P<0.05)有关。在正常体温患者(n=405)中,PCI 与 24 小时生存率增加(4.46(2.26 至 8.81),P<0.001)和 CPC 1 或 CPC 2 增加(10.81(5.86 至 19.93),P<0.001)有关。对所有患者(n=584)的进一步分析显示,MTH(7.50(4.12 至 13.65),P<0.001)和 PCI(3.88(2.11 至 7.13),P<0.001)均可增加 24 小时生存率,而 PCI 可显著增加 CPC 1 或 CPC 2 患者比例(5.66(3.54 至 9.03),P<0.001),而 MTH 则不然(1.27(0.79 至 2.03),P=0.33),尽管未调整的 Fisher 确切检验表明 MTH 有显著效果(未调整的优势比 1.83(1.23 至 2.74),P<0.05)。
PCI 可能是出院时神经功能良好(CPC 1 或 CPC 2)的独立预测因子。MTH 与更好的神经功能结果相关,尽管随后的逻辑回归分析显示 MTH 作为神经功能良好的独立预测因子没有统计学意义。因此,在成功复苏后,基于包括冠状动脉介入和低温治疗在内的标准化方案进行复苏后护理可能是有益的。主要限制之一可能是对接受 PCI 和 MTH 治疗的患者存在选择偏倚。