Department of Critical Care and the Li Ka Shing Knowledge Institute, St, Michael's Hospital, University of Toronto, 4-054C Queen Wing, 30 Bond Street, Toronto, ON M5B 1W8, Canada.
Crit Care. 2011;15(1):R69. doi: 10.1186/cc10051. Epub 2011 Feb 23.
Previous studies have documented a high frequency of endotoxemia associated with cardiopulmonary bypass (CPB). Endotoxemia may be responsible for some of the complications associated with cardiac surgery. The purpose of the study was to examine the prevalence of endotoxemia during cardiopulmonary bypass supported aortocoronary bypass grafting surgery (ACB) using a new assay, the Endotoxin Activity Assay (EAA), and explore the association between endotoxemia and post-operative infection.
The study was a single center prospective observational study measuring EAA during the perioperative period for elective ACB. Blood samples were drawn at induction of anesthesia (T1), immediately prior to release of the aortic cross-clamp (T2), and on the first post-operative morning (T3). The primary outcome was the prevalence of endotoxemia. Secondary outcomes assessed included infection rates, intensive care unit (ICU) and hospital length of stay. An EAA of < 0.40 units was interpreted as "low", 0.41 to 0.59 units as "intermediate", and ≥ 0.60 units as "high".
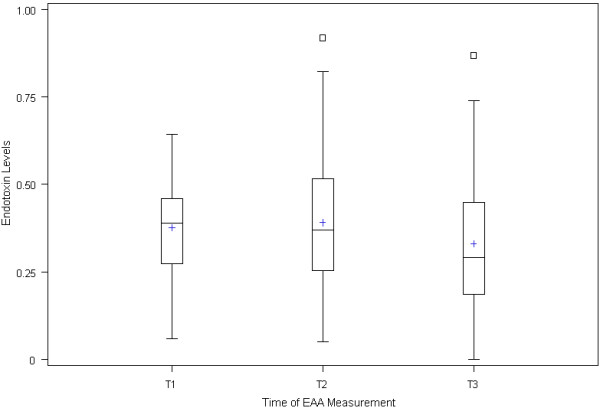
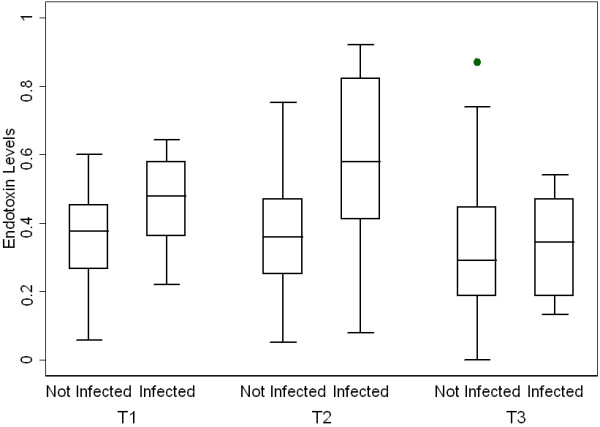
A total of 57 patients were enrolled and 54 patients were analyzable. The mean EAA at T1 was 0.38 +/- 0.14, at T2 0.39 +/- 0.18, and at T3 0.33 +/- 0.18. At T2 only 13.5% (7/52) of patients had an EAA in the high range. There was a positive correlation between EAA and duration of surgery (P = 0.02). In patients with EAA ≥ 0.40 at T2, 26.1% (6/23) of patients developed post-operative infections compared to 3.5% (1/29) of those that had a normal EAA (P = 0.0354). Maximum EAA over the first 24 hours was also strongly correlated with risk of post-operative infection (P = 0.0276).
High levels of endotoxin occur less frequently during ACB than previously documented. However, endotoxemia is associated with a significantly increased risk of the development of post-operative infection. Measuring endotoxin levels during ACB may provide a mechanism to identify and target a high risk patient population.
先前的研究记录了心肺旁路(CPB)相关的内毒素血症的高发率。内毒素血症可能是与心脏手术相关的一些并发症的原因。本研究的目的是使用新的检测方法——内毒素活性检测(EAA),检测在体外循环支持的主动脉冠状动脉旁路移植术(ACB)期间内毒素血症的发生率,并探讨内毒素血症与术后感染之间的关系。
这是一项单中心前瞻性观察研究,在选择性 ACB 的围手术期测量 EAA。在麻醉诱导时(T1)、释放主动脉夹闭前(T2)和术后第一个早晨(T3)抽取血样。主要结果是内毒素血症的发生率。次要结果评估包括感染率、重症监护病房(ICU)和住院时间。EAA<0.40 单位被解释为“低”,0.41-0.59 单位为“中”,≥0.60 单位为“高”。
共纳入 57 例患者,其中 54 例可分析。T1 时的平均 EAA 为 0.38±0.14,T2 时为 0.39±0.18,T3 时为 0.33±0.18。仅在 T2 时,13.5%(7/52)的患者 EAA 处于高范围。EAA 与手术时间呈正相关(P=0.02)。在 T2 时 EAA≥0.40 的患者中,26.1%(6/23)发生术后感染,而 EAA 正常的患者为 3.5%(1/29)(P=0.0354)。24 小时内的最大 EAA 也与术后感染的风险密切相关(P=0.0276)。
ACB 期间内毒素血症的发生率低于先前记录的水平。然而,内毒素血症与术后感染的发生风险显著增加有关。在 ACB 期间测量内毒素水平可能提供一种机制来识别和针对高危患者人群。