Department of Molecular Microbiology and Immunology, Saint Louis University School of Medicine, Saint Louis, MO 63104, USA.
Genome Med. 2011 Feb 8;3(2):8. doi: 10.1186/gm222.
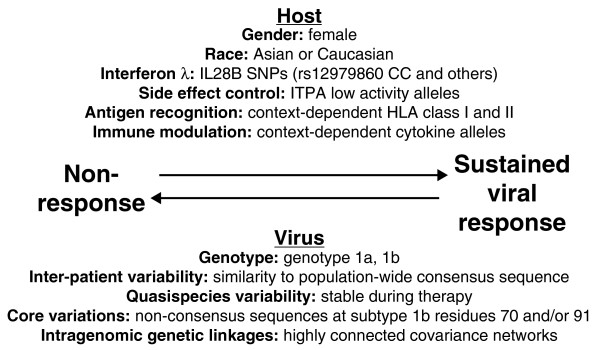
Chronic hepatitis C virus (HCV) infection is a major cause of liver disease worldwide. HCV infection is currently treated with IFNα plus ribavirin for 24 to 48 weeks. This demanding therapy fails in up to 50% of patients, so the use of pharmacogenetic biomarkers to predict the outcome of treatment would reduce futile treatment of non-responders and help identify patients in whom therapy would be justified. Both IFNα and ribavirin primarily act by modulating the immune system of the patient, and HCV uses multiple mechanisms to counteract the antiviral effects stimulated by therapy. Therefore, response to therapy is influenced by variations in human genes governing the immune system and by differences in HCV genes that blunt antiviral immune responses. This article summarizes recent advances in understanding how host and viral genetic variation affect outcome of therapy. The most notable human associations are polymorphisms within the IL28B gene, but variations in human leukocyte antigen and cytokine genes have also been associated with treatment outcome. The most prominent viral genetic association with outcome of therapy is that HCV genotype 1 is much less sensitive to treatment than genotypes 2 and 3, but genetic differences below the genotype level also influence outcome of therapy, presumably by modulating the ability of viral genes to blunt antiviral immune responses. Pharmacogenetic prediction of the outcome of IFN-based therapy for HCV will require integrating the efficacies of the immunosuppressive mechanisms of a viral isolate, and then interpreting the viral resistance potential in context of the genetic profile of the patient at loci associated with outcome of therapy. Direct-acting inhibitors of HCV that will be used in combination with IFNα are nearing approval, so genetic prediction for anti-HCV therapy will soon need to incorporate viral genetic markers of viral resistance to the new drugs.
慢性丙型肝炎病毒(HCV)感染是全球范围内导致肝脏疾病的主要原因。HCV 感染目前采用 IFNα 联合利巴韦林治疗 24 至 48 周。这种苛刻的治疗方法在多达 50%的患者中失败,因此使用药物遗传学生物标志物预测治疗结果将减少对无应答者的无效治疗,并有助于确定需要治疗的患者。IFNα 和利巴韦林主要通过调节患者的免疫系统发挥作用,而 HCV 则利用多种机制来抵消治疗刺激的抗病毒作用。因此,治疗反应受到调节免疫系统的人类基因变异和削弱抗病毒免疫反应的 HCV 基因差异的影响。本文总结了最近在理解宿主和病毒遗传变异如何影响治疗结果方面的进展。最显著的人类关联是 IL28B 基因内的多态性,但人类白细胞抗原和细胞因子基因的变异也与治疗结果相关。与治疗结果最显著的病毒遗传关联是 HCV 基因型 1对治疗的敏感性远低于基因型 2 和 3,但低于基因型水平的遗传差异也会影响治疗结果,可能是通过调节病毒基因削弱抗病毒免疫反应的能力。基于 IFN 的 HCV 治疗结果的药物遗传学预测需要整合病毒分离株的免疫抑制机制的疗效,然后根据与治疗结果相关的遗传位点上与患者遗传特征相关的病毒耐药潜力来解释。即将与 IFNα 联合使用的直接作用抗 HCV 抑制剂即将获得批准,因此抗 HCV 治疗的遗传预测很快就需要将新药物的病毒耐药性遗传标志物纳入其中。