EMGO+ Institute for Health and Care Research, Department of Public and Occupational Health, VU University Medical Center, Amsterdam, The Netherlands.
BMC Health Serv Res. 2011 Feb 28;11:49. doi: 10.1186/1472-6963-11-49.
Patient record review is believed to be the most useful method for estimating the rate of adverse events among hospitalised patients. However, the method has some practical and financial disadvantages. Some of these disadvantages might be overcome by using existing reporting systems in which patient safety issues are already reported, such as incidents reported by healthcare professionals and complaints and medico-legal claims filled by patients or their relatives. The aim of the study is to examine to what extent the hospital reporting systems cover the adverse events identified by patient record review.
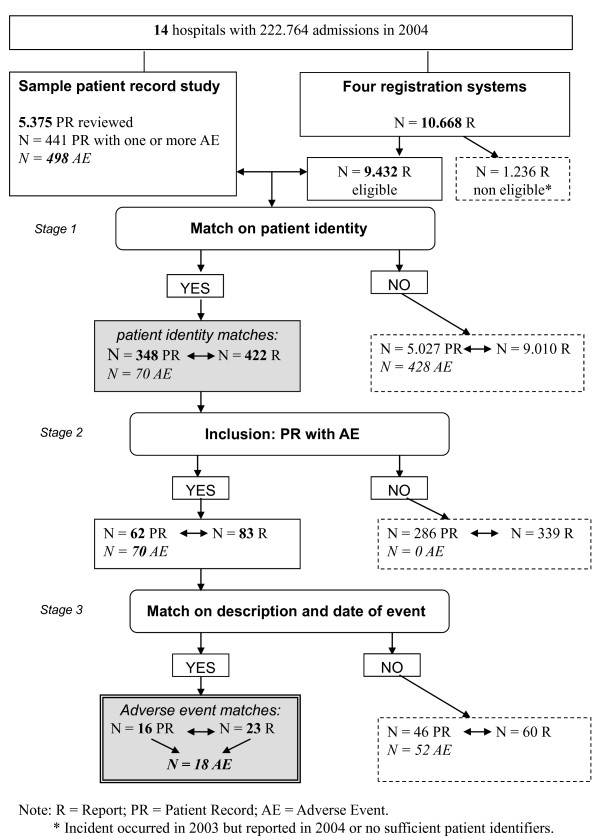
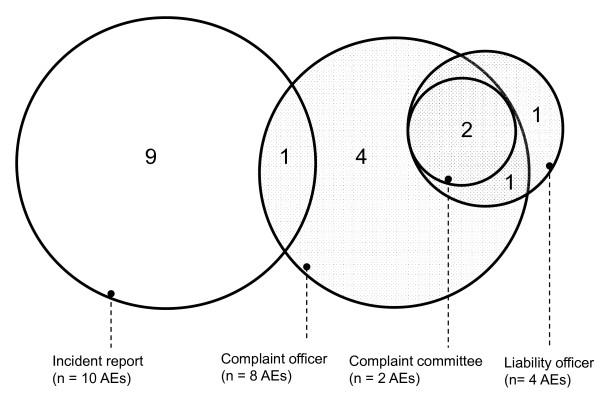
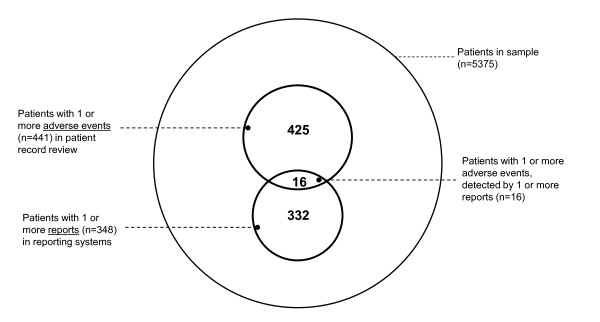
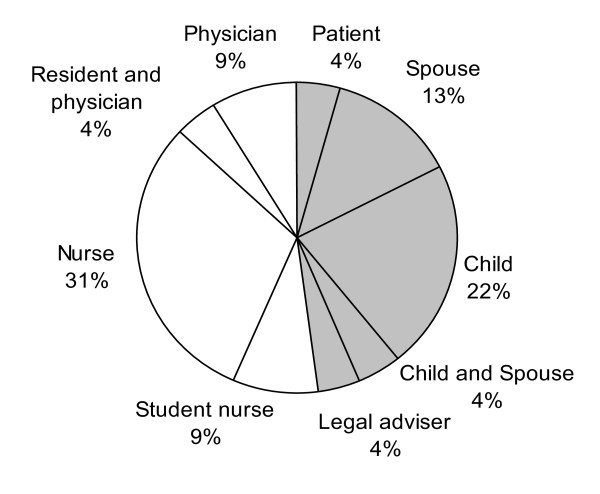
We conducted a retrospective study using a database from a record review study of 5375 patient records in 14 hospitals in the Netherlands. Trained nurses and physicians using a method based on the protocol of The Harvard Medical Practice Study previously reviewed the records. Four reporting systems were linked with the database of reviewed records: 1) informal and 2) formal complaints by patients/relatives, 3) medico-legal claims by patients/relatives and 4) incident reports by healthcare professionals. For each adverse event identified in patient records the equivalent was sought in these reporting systems by comparing dates and descriptions of the events. The study focussed on the number of adverse event matches, overlap of adverse events detected by different sources, preventability and severity of consequences of reported and non-reported events and sensitivity and specificity of reports.
In the sample of 5375 patient records, 498 adverse events were identified. Only 18 of the 498 (3.6%) adverse events identified by record review were found in one or more of the four reporting systems. There was some overlap: one adverse event had an equivalent in both a complaint and incident report and in three cases a patient/relative used two or three systems to complain about an adverse event. Healthcare professionals reported relatively more preventable adverse events than patients.Reports are not sensitive for adverse events nor do reports have a positive predictive value.
In order to detect the same adverse events as identified by patient record review, one cannot rely on the existing reporting systems within hospitals.
患者病历审查被认为是估计住院患者不良事件发生率最有用的方法。然而,该方法存在一些实际和财务上的缺点。这些缺点中的一些可以通过使用现有的报告系统来克服,这些系统已经报告了患者安全问题,例如医疗保健专业人员报告的事件、患者或其亲属提出的投诉和医疗法律索赔。本研究的目的是调查医院报告系统在多大程度上涵盖了通过患者病历审查确定的不良事件。
我们使用荷兰 14 家医院的 5375 份病历回顾研究的数据库进行了一项回顾性研究。经过培训的护士和医生使用基于哈佛医疗实践研究方案的方法对记录进行了审查。将四个报告系统与审查记录的数据库相关联:1)患者/亲属的非正式和 2)正式投诉,3)患者/亲属的医疗法律索赔,以及 4)医疗保健专业人员的事件报告。对于病历中确定的每一个不良事件,通过比较事件的日期和描述,在这些报告系统中寻找等效事件。该研究重点关注报告和未报告事件的不良事件匹配数量、不同来源检测到的不良事件的重叠、报告和未报告事件的可预防性和后果严重程度以及报告的敏感性和特异性。
在 5375 份病历样本中,确定了 498 起不良事件。仅在记录审查确定的 498 起不良事件中有 18 起(3.6%)在四个报告系统中的一个或多个系统中发现。存在一些重叠:一个不良事件在投诉和事件报告中都有等效事件,在三种情况下,患者/亲属使用两个或三个系统来投诉不良事件。医疗保健专业人员报告的可预防不良事件相对较多。报告对不良事件既不敏感,也没有阳性预测值。
为了检测与患者病历审查确定的相同的不良事件,不能仅依赖医院内现有的报告系统。