Infectious Disease Clinical Research Program, Uniformed Services University of the Health Sciences, Bethesda, MD, USA.
Vaccine. 2011 Apr 12;29(17):3183-91. doi: 10.1016/j.vaccine.2011.02.040. Epub 2011 Mar 1.
Human immunodeficiency virus (HIV)-infected persons are at risk for severe influenza infections. Although vaccination against the H1N1 pandemic influenza strain is recommended, currently there are no data on the durability of post-vaccination antibody responses in this population.
HIV-infected and HIV-uninfected adults (18-50 years old) received a single dose of monovalent 2009 influenza A (H1N1) vaccine (strain A/California/7/2009H1N1). Antibody levels to the 2009 H1N1 pandemic strain were determined at day 0, day 28, and 6 months by hemagglutination-inhibition assay. A seroprotective response was a post-vaccination titer of ≥1:40 among those with a pre-vaccination level of ≤1:10. Geometric mean titers (GMT) and factors associated with higher levels were also evaluated.
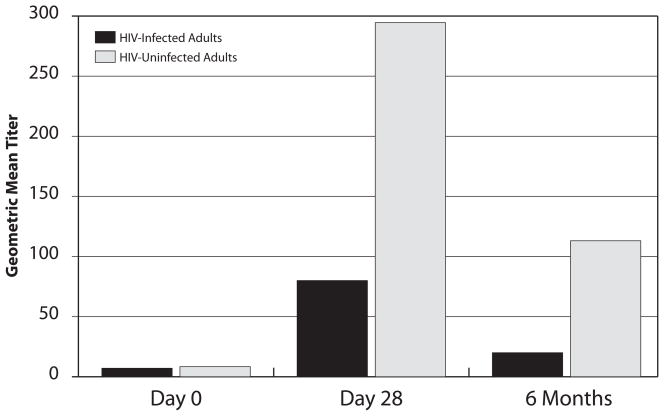
We studied 127 participants with a median age of 35 (interquartile range (IQR) 28, 42) years. Among the HIV-infected arm (n=63), the median CD4 count was 595 (IQR 476, 819)cells/mm(3) and 83% were receiving HAART. Thirty-five percent of all participants had a pre-vaccination level of >1:10. HIV-infected compared to HIV-uninfected adults were less likely to generate a seroprotective response at day 28 (54% vs. 75%, adjusted OR 0.23, p=0.021) or have a durable response at 6 months post-vaccination (28% vs. 56%, adjusted OR 0.19, p=0.005). Additionally, although pre-vaccination GMT were similar in both arms (median 7 vs. 8, p=0.11), the GMT at 6 months was significantly lower among HIV-infected versus HIV-uninfected adults (median 20 vs. 113, p=0.003). Among HIV-infected persons, younger age (p=0.035) and receipt of HAART (p=0.028) were associated with higher GMTs at 6 months.
Despite vaccination, most HIV-infected adults do not generate durable seroprotective antibody responses to the 2009 influenza A (H1N1) virus, and hence may remain vulnerable to infection. In addition to HAART use, more immunogenic vaccines are likely needed for improving protection against influenza in this population.
感染人类免疫缺陷病毒(HIV)的人有发生严重流感感染的风险。尽管推荐接种针对 H1N1 大流行流感株的疫苗,但目前尚无关于该人群接种后抗体反应持久性的数据。
HIV 感染和未感染的成年人(18-50 岁)接受了一剂单价 2009 年甲型流感(H1N1)疫苗(A/California/7/2009H1N1 株)。通过血凝抑制试验在第 0 天、第 28 天和 6 个月时测定对 2009 年 H1N1 大流行株的抗体水平。接种疫苗后的血清保护反应是指接种前滴度≤1:10 的人群接种后的滴度≥1:40。还评估了几何平均滴度(GMT)和与较高水平相关的因素。
我们研究了 127 名中位年龄为 35 岁(四分位间距 28,42)的参与者。在 HIV 感染组(n=63)中,中位 CD4 计数为 595(四分位间距 476,819)细胞/mm3,83%正在接受 HAART。所有参与者中有 35%接种前的滴度>1:10。与 HIV 未感染成年人相比,HIV 感染成年人在第 28 天产生血清保护反应的可能性较小(54% vs. 75%,调整后的 OR 0.23,p=0.021),或在接种疫苗后 6 个月时产生持久反应的可能性较小(28% vs. 56%,调整后的 OR 0.19,p=0.005)。此外,尽管两臂接种前 GMT 相似(中位数 7 与 8,p=0.11),但 HIV 感染组与 HIV 未感染组相比,6 个月时的 GMT 显著较低(中位数 20 与 113,p=0.003)。在 HIV 感染人群中,年龄较小(p=0.035)和接受 HAART(p=0.028)与 6 个月时较高的 GMT 相关。
尽管进行了疫苗接种,但大多数 HIV 感染成年人对 2009 年甲型流感(H1N1)病毒不会产生持久的血清保护抗体反应,因此仍可能容易受到感染。除了使用 HAART 外,还可能需要更具免疫原性的疫苗来改善该人群对流感的保护。