Section of Medicine, The Institute of Cancer Research and Royal Marsden NHS Foundation Trust, Sutton, Surrey, United Kingdom.
Clin Cancer Res. 2011 Apr 1;17(7):1649-57. doi: 10.1158/1078-0432.CCR-10-0567. Epub 2011 Mar 3.
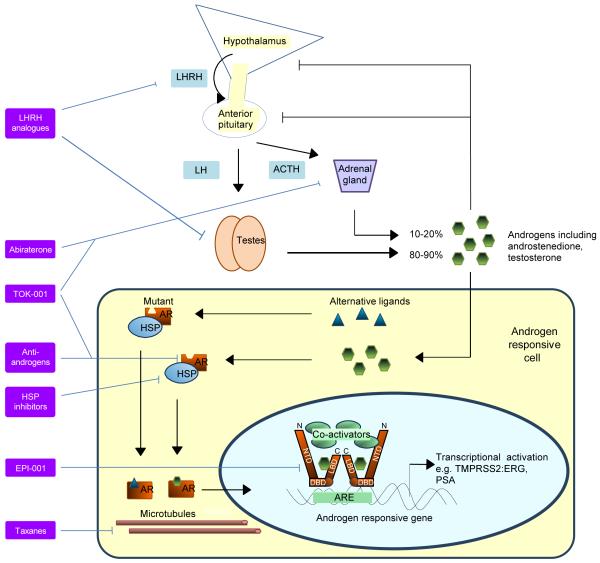
Recent data report that abiraterone acetate, a specific inhibitor of CYP17 that is key to androgen and estrogen synthesis, improves survival in metastatic castration-resistant prostate cancer (CRPC), confirming the continued dependency of CRPC on the androgen receptor (AR) signaling pathway. MDV3100 is a novel antagonist of AR that is also in phase III clinical trials. In addition, several other agents targeting the AR axis are undergoing evaluation in early clinical studies. CRPC patients progress on these therapies with an increasing prostate specific antigen (PSA), suggesting that repeated therapeutic interventions targeting the AR signaling axis could induce secondary responses and achieve prolonged clinical benefit for a subgroup of patients. These exciting results are good news for patients but introduce a number of treatment paradigm dilemmas for physicians. Clinical studies evaluating the ideal sequence of administration of these new agents, best timing for initiation, combination strategies, discontinuation beyond progression and after commencement of subsequent therapies, and coordination with other treatments have not been done. Predictive biomarkers could allow patient selection for a specific treatment, but in their absence, most physicians will rely on a trial of treatment with a preferred agent and substitute for an alternative therapy on objective progression. Current data suggest that the response rate to drugs targeting the AR ligand-binding domain decreases with each treatment, but we hypothesize that a significant proportion of CRPC remains dependent on the AR axis and, therefore, novel strategies for disrupting AR signaling merit evaluation.
最近的数据报告表明,CYP17 的特异性抑制剂醋酸阿比特龙能够改善转移性去势抵抗性前列腺癌(CRPC)患者的生存,这证实了 CRPC 仍然依赖于雄激素受体(AR)信号通路。MDV3100 是一种新型的 AR 拮抗剂,也正在进行 III 期临床试验。此外,还有其他几种针对 AR 轴的药物正在早期临床研究中进行评估。CRPC 患者在这些治疗中会出现前列腺特异性抗原(PSA)水平升高,这表明针对 AR 信号轴的重复治疗干预可能会引发继发性反应,并为一部分患者带来长期的临床获益。这些令人兴奋的结果对患者来说是个好消息,但也给医生带来了许多治疗模式的困境。目前还没有研究评估这些新药物的理想给药顺序、最佳起始时间、联合策略、进展后停药以及开始后续治疗后的停药策略,以及与其他治疗方法的协调。预测性生物标志物可以帮助患者选择特定的治疗方法,但在缺乏生物标志物的情况下,大多数医生将依赖于首选药物的治疗试验,并在客观进展时替代其他治疗方法。目前的数据表明,针对 AR 配体结合域的药物的反应率随着每次治疗而降低,但我们假设,相当一部分 CRPC 仍然依赖于 AR 轴,因此,破坏 AR 信号的新策略值得评估。