Medical Intensive Care Unit and Biostatistics Departments, Saint-Louis Teaching Hospital, 1 avenue Claude Vellefaux, Paris F-75010, France.
Crit Care. 2011;15(2):R91. doi: 10.1186/cc10091. Epub 2011 Mar 8.
Data on pulmonary complications in renal transplant recipients are scarce. The aim of this study was to evaluate acute respiratory failure (ARF) in renal transplant recipients.
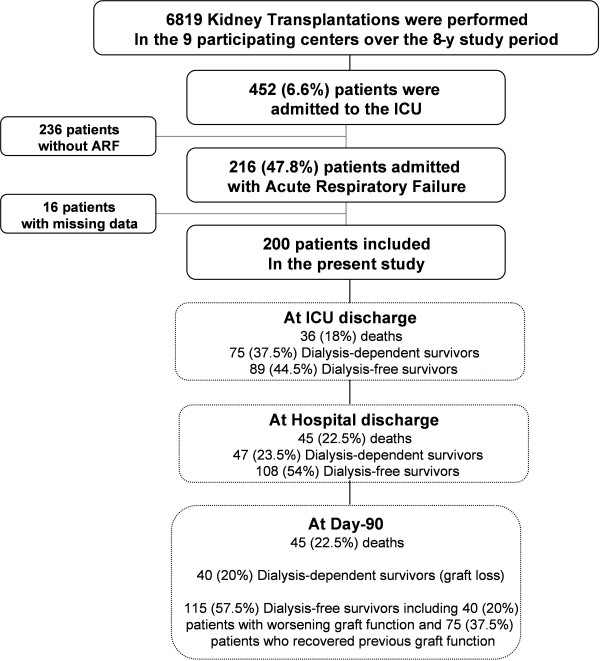
We conducted a retrospective observational study in nine transplant centers of consecutive kidney transplant recipients admitted to the intensive care unit (ICU) for ARF from 2000 to 2008.
Of 6,819 kidney transplant recipients, 452 (6.6%) required ICU admission, including 200 admitted for ARF. Fifteen (7.5%) of these patients had combined kidney-pancreas transplantations. The most common causes of ARF were bacterial pneumonia (35.5%), cardiogenic pulmonary edema (24.5%) and extrapulmonary acute respiratory distress syndrome (ARDS) (15.5%). Pneumocystis pneumonia occurred in 11.5% of patients. Mechanical ventilation was used in 93 patients (46.5%), vasopressors were used in 82 patients (41%) and dialysis was administered in 104 patients (52%). Both the in-hospital and 90-day mortality rates were 22.5%. Among the 155 day 90 survivors, 115 patients (74.2%) were dialysis-free, including 75 patients (65.2%) who recovered prior renal function. Factors independently associated with in-hospital mortality were shock at admission (odds ratio (OR) 8.70, 95% confidence interval (95% CI) 3.25 to 23.29), opportunistic fungal infection (OR 7.08, 95% CI 2.32 to 21.60) and bacterial infection (OR 2.53, 95% CI 1.07 to 5.96). Five factors were independently associated with day 90 dialysis-free survival: renal Sequential Organ Failure Assessment (SOFA) score on day 1 (OR 0.68/SOFA point, 95% CI 0.52 to 0.88), bacterial infection (OR 0.43, 95% CI 0.21 to 0.90), three or four quadrants involved on chest X-ray (OR 0.44, 95% CI 0.21 to 0.91), time from hospital to ICU admission (OR 0.98/day, 95% CI 0.95 to 0.99) and oxygen flow at admission (OR 0.93/liter, 95% CI 0.86 to 0.99).
In kidney transplant recipients, ARF is associated with high mortality and graft loss rates. Increased Pneumocystis and bacterial prophylaxis might improve these outcomes. Early ICU admission might prevent graft loss.
有关肾移植受者肺部并发症的数据很少。本研究的目的是评估肾移植受者急性呼吸衰竭(ARF)。
我们在 2000 年至 2008 年期间对 9 个移植中心的连续肾移植受者进行了回顾性观察性研究,这些受者因 ARF 而被收入重症监护病房(ICU)。
在 6819 例肾移植受者中,有 452 例(6.6%)需要 ICU 入院,其中 200 例因 ARF 入院。这些患者中有 15 例(7.5%)接受了肾胰联合移植。ARF 的最常见原因是细菌性肺炎(35.5%),心源性肺水肿(24.5%)和肺外急性呼吸窘迫综合征(ARDS)(15.5%)。11.5%的患者发生卡氏肺孢子虫肺炎。93 例患者(46.5%)使用机械通气,82 例患者(41%)使用血管加压素,104 例患者(52%)接受透析。院内和 90 天死亡率均为 22.5%。在 155 名 90 天幸存者中,有 115 名(74.2%)无需透析,其中 75 名(65.2%)恢复了先前的肾功能。与院内死亡率相关的独立因素为入院时休克(优势比(OR)8.70,95%置信区间(95%CI)3.25 至 23.29),机会性真菌感染(OR 7.08,95%CI 2.32 至 21.60)和细菌感染(OR 2.53,95%CI 1.07 至 5.96)。有五个因素与第 90 天无透析存活率独立相关:第 1 天的肾脏序贯器官衰竭评估(SOFA)评分(OR 0.68/SOFA 点,95%CI 0.52 至 0.88),细菌感染(OR 0.43,95%CI 0.21 至 0.90),胸部 X 线检查涉及三个或四个象限(OR 0.44,95%CI 0.21 至 0.91),从医院到 ICU 入院的时间(OR 0.98/天,95%CI 0.95 至 0.99)和入院时的氧气流量(OR 0.93/升,95%CI 0.86 至 0.99)。
在肾移植受者中,ARF 与高死亡率和移植物丢失率相关。增加卡氏肺孢子虫和细菌预防可能会改善这些结果。早期 ICU 入院可能会防止移植物丢失。