Fiorentino Marco, Bagagli Francesca, Deleonardis Annamaria, Stasi Alessandra, Franzin Rossana, Conserva Francesca, Infante Barbara, Stallone Giovanni, Pontrelli Paola, Gesualdo Loreto
Nephrology, Dialysis and Transplantation Unit, Department of Precision and Regenerative Medicine and Ionian Area (DiMePRe-J), University of Bari "Aldo Moro", 70121 Bari, Italy.
Nephrology, Dialysis and Transplantation Unit, Department of Medical and Surgical Science, University of Foggia, 71122 Foggia, Italy.
Biomedicines. 2023 May 18;11(5):1474. doi: 10.3390/biomedicines11051474.
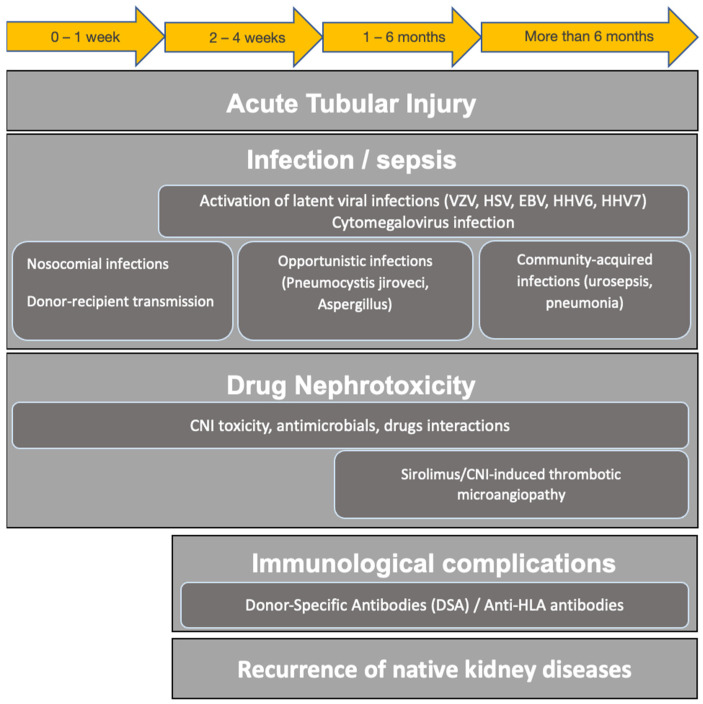
Kidney transplantation is the first-choice treatment for end-stage renal disease (ESRD). Kidney transplant recipients (KTRs) are at higher risk of experiencing a life-threatening event requiring intensive care unit (ICU) admission, mainly in the late post-transplant period (more than 6 months after transplantation). Urosepsis and bloodstream infections account for almost half of ICU admissions in this population; in addition, potential side effects related to immunosuppressive treatment should be accounted for cytotoxic and ischemic changes induced by calcineurin inhibitor (CNI), sirolimus/CNI-induced thrombotic microangiopathy and posterior reversible encephalopathy syndrome. Throughout the ICU stay, Acute Kidney Injury (AKI) incidence is common and ranges from 10% to 80%, and up to 40% will require renal replacement therapy. In-hospital mortality can reach 30% and correlates with acute illness severity and admission diagnosis. Graft survival is subordinated to baseline estimated glomerular filtration rate (eGFR), clinical presentation, disease severity and potential drug nephrotoxicity. The present review aims to define the impact of AKI events on short- and long-term outcomes in KTRs, focusing on the epidemiologic data regarding AKI incidence in this subpopulation; the pathophysiological mechanisms underlying AKI development and potential AKI biomarkers in kidney transplantation, graft and patients' outcomes; the current diagnostic work up and management of AKI; and the modulation of immunosuppression in ICU-admitted KTRs.
肾移植是终末期肾病(ESRD)的首选治疗方法。肾移植受者(KTRs)发生危及生命事件而需要入住重症监护病房(ICU)的风险更高,主要发生在移植后期(移植后6个月以上)。泌尿系统感染和血流感染占该人群ICU入院病例的近一半;此外,免疫抑制治疗的潜在副作用应考虑为钙调神经磷酸酶抑制剂(CNI)引起的细胞毒性和缺血性改变、西罗莫司/CNI诱导的血栓性微血管病和后部可逆性脑病综合征。在整个ICU住院期间,急性肾损伤(AKI)的发生率很常见,范围从10%到80%,高达40%的患者需要肾脏替代治疗。住院死亡率可达30%,并与急性疾病严重程度和入院诊断相关。移植肾存活取决于基线估计肾小球滤过率(eGFR)、临床表现、疾病严重程度和潜在的药物肾毒性。本综述旨在确定AKI事件对KTRs短期和长期预后的影响,重点关注该亚人群中AKI发生率的流行病学数据;肾移植中AKI发生的病理生理机制和潜在的AKI生物标志物、移植肾和患者的预后;目前AKI的诊断检查和管理;以及入住ICU的KTRs免疫抑制的调整。