Department of Global Health, University of Washington, Seattle, Washington, USA.
PLoS Med. 2011 Mar;8(3):e1000422. doi: 10.1371/journal.pmed.1000422. Epub 2011 Mar 1.
Behavioral interventions that promote adherence to antiretroviral medications may decrease HIV treatment failure. Antiretroviral treatment programs in sub-Saharan Africa confront increasing financial constraints to provide comprehensive HIV care, which include adherence interventions. This study compared the impact of counseling and use of an alarm device on adherence and biological outcomes in a resource-limited setting.
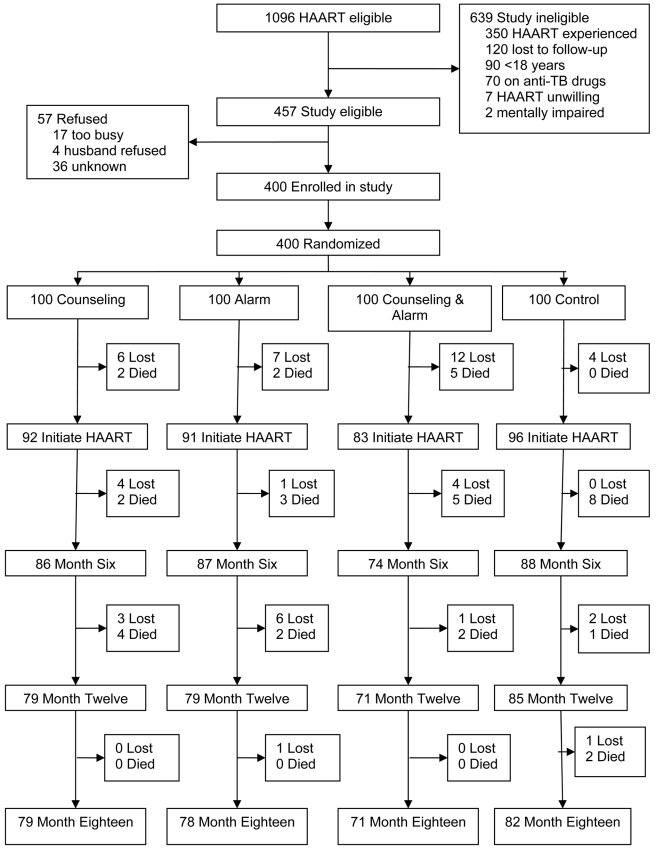
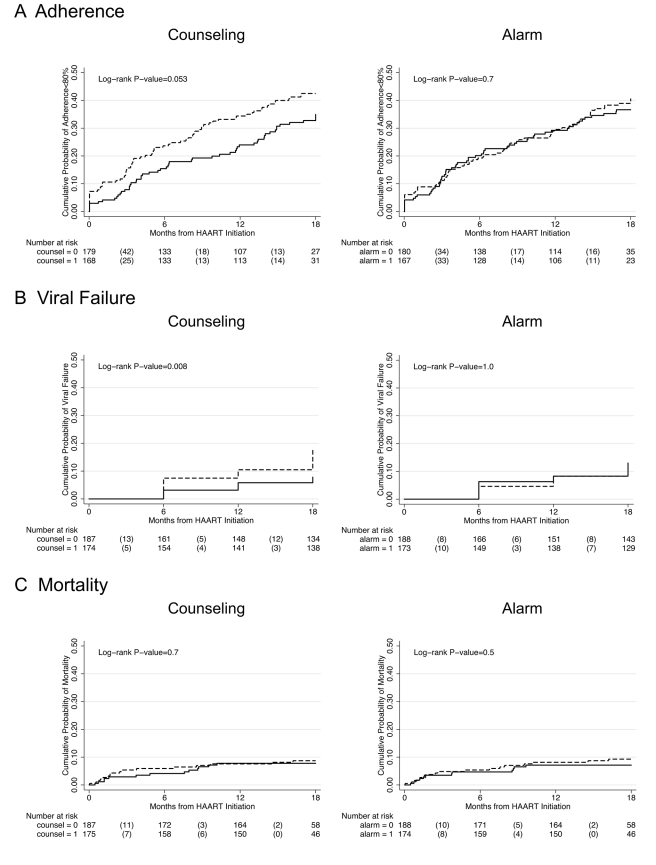
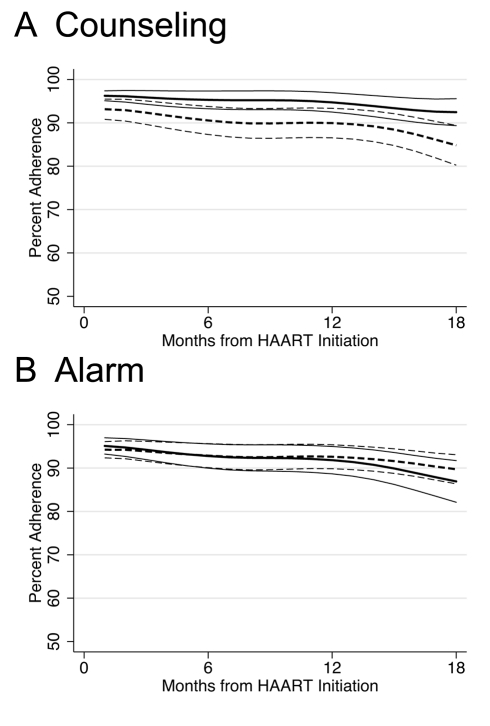
A randomized controlled, factorial designed trial was conducted in Nairobi, Kenya. Antiretroviral-naïve individuals initiating free highly active antiretroviral therapy (HAART) in the form of fixed-dose combination pills (d4T, 3TC, and nevirapine) were randomized to one of four arms: counseling (three counseling sessions around HAART initiation), alarm (pocket electronic pill reminder carried for 6 months), counseling plus alarm, and neither counseling nor alarm. Participants were followed for 18 months after HAART initiation. Primary study endpoints included plasma HIV-1 RNA and CD4 count every 6 months, mortality, and adherence measured by monthly pill count. Between May 2006 and September 2008, 400 individuals were enrolled, 362 initiated HAART, and 310 completed follow-up. Participants who received counseling were 29% less likely to have monthly adherence <80% (hazard ratio [HR] = 0.71; 95% confidence interval [CI] 0.49-1.01; p = 0.055) and 59% less likely to experience viral failure (HIV-1 RNA ≥5,000 copies/ml) (HR 0.41; 95% CI 0.21-0.81; p = 0.01) compared to those who received no counseling. There was no significant impact of using an alarm on poor adherence (HR 0.93; 95% CI 0.65-1.32; p = 0.7) or viral failure (HR 0.99; 95% CI 0.53-1.84; p = 1.0) compared to those who did not use an alarm. Neither counseling nor alarm was significantly associated with mortality or rate of immune reconstitution.
Intensive early adherence counseling at HAART initiation resulted in sustained, significant impact on adherence and virologic treatment failure during 18-month follow-up, while use of an alarm device had no effect. As antiretroviral treatment clinics expand to meet an increasing demand for HIV care in sub-Saharan Africa, adherence counseling should be implemented to decrease the development of treatment failure and spread of resistant HIV.
促进抗逆转录病毒药物依从性的行为干预措施可能会降低 HIV 治疗失败的风险。撒哈拉以南非洲的抗逆转录病毒治疗项目面临着越来越大的提供全面 HIV 护理的财政限制,其中包括依从性干预措施。本研究比较了咨询和使用报警装置对资源有限环境下的依从性和生物学结果的影响。
这是在肯尼亚内罗毕进行的一项随机对照、析因设计试验。接受固定剂量复方片剂(d4T、3TC 和奈韦拉平)的抗逆转录病毒初治个体开始免费高效抗逆转录病毒治疗(HAART),随机分为以下四个组之一:咨询(HAART 启动前后进行三次咨询)、报警(携带电子药丸提醒器 6 个月)、咨询加报警和既不咨询也不报警。参与者在 HAART 启动后随访 18 个月。主要研究终点包括每 6 个月进行一次血浆 HIV-1 RNA 和 CD4 计数、死亡率以及每月药物计数衡量的依从性。2006 年 5 月至 2008 年 9 月期间,共纳入 400 名参与者,其中 362 名开始 HAART,310 名完成随访。接受咨询的参与者每月的依从性<80%的可能性降低了 29%(风险比 [HR] = 0.71;95%置信区间 [CI] 0.49-1.01;p = 0.055),病毒失败(HIV-1 RNA≥5,000 拷贝/ml)的可能性降低了 59%(HR 0.41;95% CI 0.21-0.81;p = 0.01)。与未接受咨询的参与者相比,使用报警装置对不良依从性(HR 0.93;95% CI 0.65-1.32;p = 0.7)或病毒失败(HR 0.99;95% CI 0.53-1.84;p = 1.0)没有显著影响。与未使用报警装置的参与者相比,既不咨询也不报警对死亡率或免疫重建率均无显著影响。
在 HAART 启动时进行强化早期依从性咨询,在 18 个月的随访中对依从性和病毒学治疗失败产生了持续的显著影响,而使用报警装置则没有效果。随着抗逆转录病毒治疗诊所的扩大,以满足撒哈拉以南非洲地区对 HIV 护理日益增长的需求,应实施依从性咨询,以降低治疗失败和耐药性 HIV 的传播。