Pediatric Endocrine Unit, Dept. of Pediatrics, Makarios Hospital, Nicosia, Cyprus.
Mediterr J Hematol Infect Dis. 2009 Jul 27;1(1):e2009003. doi: 10.4084/MJHID.2009.003.
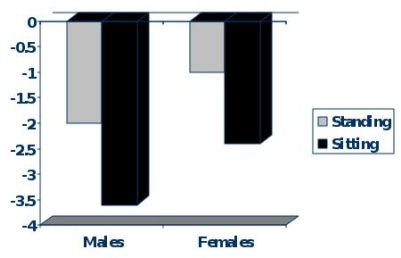
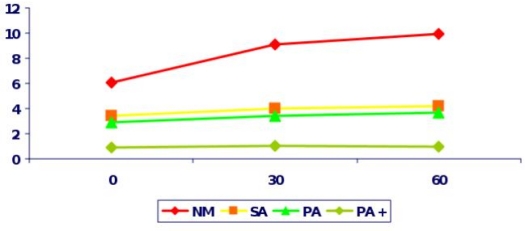
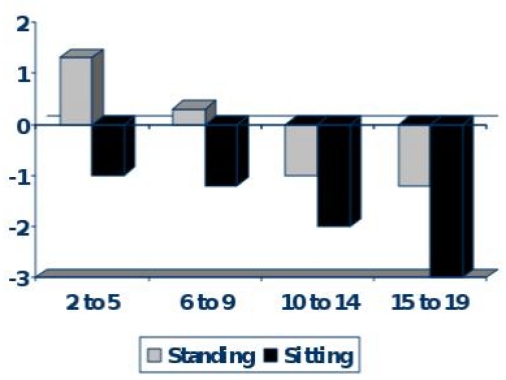
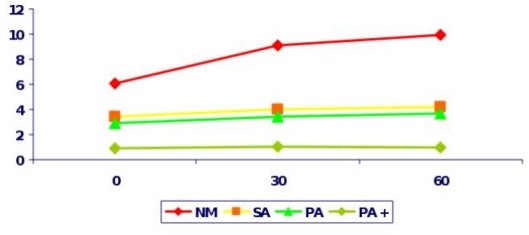
Endocrine dysfunction in Thalassaemia major (TM) is a common and disturbing complication, which requires prompt recognition and treatment. The contribution of the underlying molecular defect in TM to the development of endocrinopathies is significant because the patients with the more severe genetic defects have a greater rate of iron loading through higher red cell consumption. TM patients frequently present delay of growth and puberty with reduction of final height. The pathogenesis of growth failure is multifactorial and is mainly due to chronic anemia and hypoxia, chronic liver disease, zinc and folic acid deficiency, iron overload, intensive use of chelating agents, emotional factors, and endocrinopathies (hypogonadism, delayed puberty, hypothyroidism) and GH-IGF-1 axis dysregulation. Although appropriate iron chelation therapy can improve growth and development, TM children and adolescents treated intensively with desferrioxamine remain short as well, showing body disproportion between the upper and lower body segment. Body disproportion is independent of pubertal or prepubertal period of greater height gain. Treatment with recombinant GH (rhGH) is recommended when GH deficiency is established, and even so, the therapeutic response is often non satisfactory. Growth acceleration is mostly promoted with sex steroids in children with associated pubertal delay. Sexual complications in TM, which include Delayed Puberty, Arrested Puberty and Hypogonadism, present the commonest endocrine complication. Iron deposition on gonadotroph cells of the pituitary leads to disruption of gonadotrophin production which is proven by the poor response of FSH and LH to GnRH stimulation. In the majority of patients gonadal function is normal as most women with Amenorrhea are capable of achieving pregnancy with hormonal treatment and similarly men with azoospermia become fathers. Secondary Hypogonadism appears later in life, and is manifested in women as Secondary Amenorrhea and in men as decline in sexual drive and azzoospermia. The damage to the hypothalamus and pituitary is progressive, even when intensive chelating therapy is given and the appearance of Hypogonadism in both sexes is often unavoidable. Close follow up and proper management is crucial for every patient with TM. Early recognition of growth disturbance and prevention of hypogonadism by early and judicious chelation therapy is mandatory for the improvement of their quality of life. Patients with TM can now live a better life due to modern advances in their medical care and our better understanding in the pathogenesis, manifestation and prevention of endocrine complications.
地中海贫血(TM)患者存在常见且令人困扰的内分泌功能紊乱,需要及时识别和治疗。TM 患者的严重程度与基因缺陷有关,这些患者由于红细胞的过度消耗,铁负荷量更大,因此更易发生内分泌疾病。TM 患者经常表现为生长和青春期延迟,最终身高降低。生长障碍的发病机制是多因素的,主要与慢性贫血和缺氧、慢性肝病、锌和叶酸缺乏、铁过载、螯合剂的大量使用、情绪因素以及内分泌疾病(性腺功能减退症、青春期延迟、甲状腺功能减退症)和 GH-IGF-1 轴失调有关。尽管适当的铁螯合治疗可以改善生长发育,但接受去铁胺强化治疗的 TM 儿童和青少年仍然身材矮小,表现为上下半身比例失调。这种比例失调与青春期或青春期前身高增长高峰期无关。当确定存在生长激素缺乏症时,推荐使用重组人生长激素(rhGH)治疗,但治疗反应通常并不理想。对于伴有青春期延迟的儿童,主要使用性激素促进生长加速。TM 患者还存在性并发症,包括青春期延迟、青春期停止和性腺功能减退症,是最常见的内分泌并发症。铁沉积在垂体的促性腺细胞上,导致促性腺激素的产生中断,这可以通过 FSH 和 LH 对 GnRH 刺激的反应不良来证明。在大多数患者中,性腺功能正常,因为大多数闭经的女性可以通过激素治疗怀孕,同样,无精子症的男性也可以成为父亲。继发性性腺功能减退症在以后的生活中出现,女性表现为继发性闭经,男性表现为性欲下降和无精子症。即使给予强化螯合治疗,下丘脑和垂体的损伤也是进行性的,男女两性的性腺功能减退症通常不可避免。对于每一位 TM 患者,密切随访和适当的管理至关重要。早期识别生长障碍,通过早期和明智的螯合治疗预防性腺功能减退症,对于提高他们的生活质量至关重要。由于现代医疗的进步以及我们对内分泌并发症的发病机制、表现和预防的更好理解,TM 患者现在可以过上更好的生活。