Celera, 1401 Harbor Bay Parkway, Alameda, CA 94502, USA.
BMC Med Genet. 2011 Mar 24;12:42. doi: 10.1186/1471-2350-12-42.
Case-control studies typically exclude fatal endpoints from the case set, which we hypothesize will substantially underestimate risk if survival is genotype-dependent. The loss of fatal cases is particularly nontrivial for studies of coronary heart disease (CHD) because of significantly reduced survival (34% one-year fatality following a coronary attack). A case in point is the KIF6 Trp719Arg polymorphism (rs20455). Whereas six prospective studies have shown that carriers of the KIF6 Trp719Arg risk allele have 20% to 50% greater CHD risk than non-carriers, several cross-sectional case-control studies failed to show that carrier status is related to CHD. Computer simulations were therefore employed to assess the impact of the loss of fatal events on gene associations in cross-sectional case-control studies, using KIF6 Trp719Arg as an example.
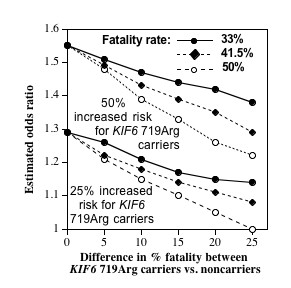
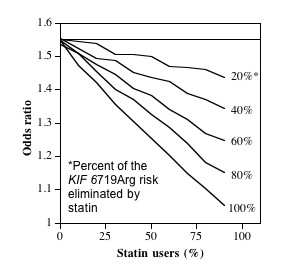
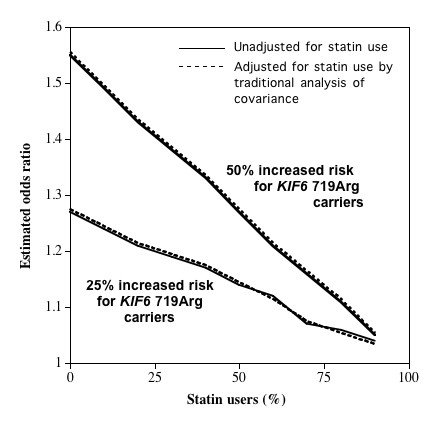
Ten replicates of 1,000,000 observations each were generated reflecting Canadian demographics. Cardiovascular disease (CVD) risks were assigned by the Framingham equation and events distributed among KIF6 Trp719Arg genotypes according to published prospective studies. Logistic regression analysis was used to estimate odds ratios between KIF6 genotypes. Results were examined for 33%, 41.5%, and 50% fatality rates for incident CVD.In the absence of any difference in percent fatalities between genotypes, the odds ratios (carriers vs. noncarriers) were unaffected by survival bias, otherwise the odds ratios were increasingly attenuated as the disparity between fatality rates increased between genotypes. Additional simulations demonstrated that statin usage, shown in four clinical trials to substantially reduce the excess CHD risk in the KIF6 719Arg variant, should also attenuate the KIF6 719Arg odds ratio in case-control studies.
These computer simulations show that exclusions of prior CHD fatalities attenuate odds ratios of case-control studies in proportion to the difference in the percent fatalities between genotypes. Disproportionate CHD survival for KIF6 Trip719Arg carriers is suggested by their 50% greater risk for recurrent myocardial infarction. This, and the attenuation of KIF6 719Arg carrier risk with statin use, may explain the genotype's weak association with CHD in cross-sectional case-control studies. The results may be relevant to the underestimation of risk in cross-sectional case-control studies of other genetic CHD-risk factors affecting survival.
病例对照研究通常将病例组中的致死终点排除在外,如果生存与基因型相关,我们假设这将大大低估风险。对于冠心病(CHD)研究,由于生存率显著降低(冠状动脉发作后一年的死亡率为 34%),因此失去致死病例尤其重要。一个典型的例子是 KIF6 Trp719Arg 多态性(rs20455)。虽然六项前瞻性研究表明,KIF6 Trp719Arg 风险等位基因的携带者比非携带者患 CHD 的风险高 20%至 50%,但几项横断面病例对照研究未能表明携带者状态与 CHD 相关。因此,使用 KIF6 Trp719Arg 作为示例,我们通过计算机模拟来评估在横断面病例对照研究中,因失去致死事件而对基因相关性的影响。
生成了 100 万个观察值的 10 个重复,反映了加拿大的人口统计学特征。心血管疾病(CVD)风险由 Framingham 方程分配,根据已发表的前瞻性研究,将事件分布在 KIF6 Trp719Arg 基因型之间。使用逻辑回归分析估计 KIF6 基因型之间的优势比。对于 CVD 发生率为 33%、41.5%和 50%的病死率,检查了结果。在基因型之间无病死率差异的情况下,优势比(携带者与非携带者)不受生存偏差的影响,否则,随着基因型之间病死率差异的增加,优势比逐渐减弱。额外的模拟表明,四项临床试验表明他汀类药物的使用可大大降低 KIF6 719Arg 变异体中 CHD 风险的增加,也应降低病例对照研究中 KIF6 719Arg 的优势比。
这些计算机模拟表明,由于基因型之间病死率的差异,排除先前的 CHD 致死病例会按比例减弱病例对照研究的优势比。KIF6 Trip719Arg 携带者的 CHD 生存不均衡,提示他们再次发生心肌梗死的风险增加了 50%。这一点以及他汀类药物的使用降低了 KIF6 719Arg 携带者的风险,可能解释了 KIF6 719Arg 与 CHD 在横断面病例对照研究中的弱相关性。这些结果可能与其他影响生存的遗传 CHD 风险因素的横断面病例对照研究中风险的低估有关。