Lapice Emanuela, Monticelli Antonella, Cocozza Sergio, Pinelli Michele, Cocozza Sara, Bruzzese Dario, Riccardi Gabriele, Vaccaro Olga
Department of Clinical Medicine and Surgery, University of Naples Federico II, Via S Pansini 5, Naples, 80131, Italy.
Department of Cellular and Molecular Biology and Pathology A. Califano DBPCM, University of Naples Federico II, Via S Pansini 5, Naples, 80131, Italy.
J Transl Med. 2015 Mar 12;13:85. doi: 10.1186/s12967-015-0448-6.
Cross-sectional studies suggest the association between diabetic nephropathy and the PPARγ2 Pro12Ala polymorphism of the peroxisome proliferator-activated receptor γ2 (PPARγ2). Prospective data are limited to microalbuminuria and no information on renal function is available to date. The present study evaluates the association between the Pro12Ala polymorphism of PPARγ2 and the progression of albuminuria and decay in glomerular filtration rate (GFR) in type 2 diabetes.
We studied 256 patients with an average 5-year follow-up. Among others, urinary albumin excretion rate (UAER) was measured on spot sample, GFR was estimated with the CKD-EPI Equation.
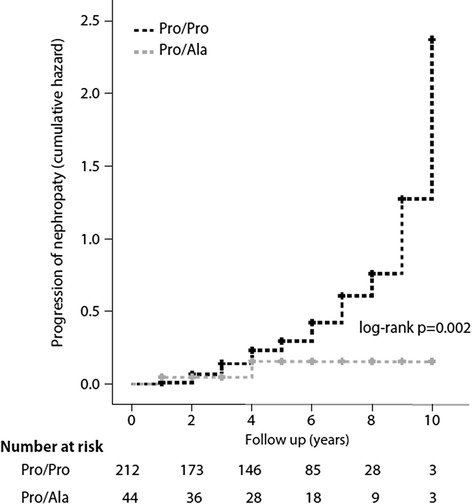
Baseline UAER and GFR were similar for carriers or non-carriers of the polymorphism. At follow-up no significant changes from baseline were observed for UAER or eGFR in carriers of the Pro12Ala polymorphism whereas a significant increase in UAER [17 (11.3-37.9) versus 24.5 (13.8-49.9) μg/mg, p < 0.006)] and a significant reduction in the eGFR (82.8 ± 14.5 versus 80.3 ± 17.3 ml/min/1.73, m(2) p = 0.02), were observed in non carriers of the Pro12Ala polymorphism. Progression of nephropathy - defined according to a combined end point of UAER and eGFR- i.e. doubling of baseline UAER to at least 100 μg/mg, or new onset microalbuminuria, or progression from micro to macroalbuminuria, or 25% reduction of eGFR, or annualized eGFR decline >3 ml/min/year - was significantly less frequent in Ala carriers than non carriers (11.4% vs 35.8%; p < 0.01); HR adjusted for baseline age, AER, eGFR, HbA1c, diabetes duration and blood pressure was 0.32 (0.12-0.80).
This study found that among patients with type 2 diabetes, the PPARγ2 Pro12Ala polymorphism is protective against progression of nephropathy and decay of renal function independent of major confounders.
横断面研究提示糖尿病肾病与过氧化物酶体增殖物激活受体γ2(PPARγ2)的PPARγ2 Pro12Ala多态性之间存在关联。前瞻性数据仅限于微量白蛋白尿,且迄今为止尚无关于肾功能的信息。本研究评估PPARγ2的Pro12Ala多态性与2型糖尿病患者蛋白尿进展及肾小球滤过率(GFR)下降之间的关联。
我们研究了256例患者,平均随访5年。除其他指标外,采用即时尿样测量尿白蛋白排泄率(UAER),用慢性肾脏病流行病学协作组(CKD-EPI)公式估算GFR。
该多态性的携带者与非携带者的基线UAER和GFR相似。在随访期间,Pro12Ala多态性携带者的UAER或估算肾小球滤过率(eGFR)与基线相比无显著变化,而Pro12Ala多态性非携带者的UAER显著升高[17(11.3 - 37.9)对24.5(13.8 - 49.9)μg/mg,p < 0.006],eGFR显著降低(82.8 ± 14.5对80.3 ± 17.3 ml/min/1.73 m²,p = 0.02)。根据UAER和eGFR的综合终点定义的肾病进展,即基线UAER翻倍至至少100 μg/mg,或新发微量白蛋白尿,或从微量白蛋白尿进展为大量白蛋白尿,或eGFR降低25%,或年化eGFR下降>3 ml/min/年,Ala携带者的发生率显著低于非携带者(11.4%对35.8%;p < 0.01);根据基线年龄、AER、eGFR、糖化血红蛋白、糖尿病病程和血压调整后的风险比为0.32(0.12 - 0.80)。
本研究发现,在2型糖尿病患者中,PPARγ2 Pro12Ala多态性可独立于主要混杂因素,对肾病进展和肾功能衰退起到保护作用。