Abramson Cancer Center, Hospital of the University of Pennsylvania, Philadelphia, PA, USA.
Bone Marrow Transplant. 2012 Feb;47(2):203-11. doi: 10.1038/bmt.2011.69. Epub 2011 Mar 28.
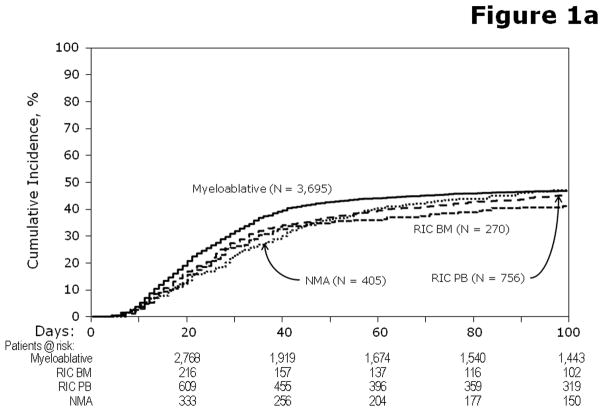
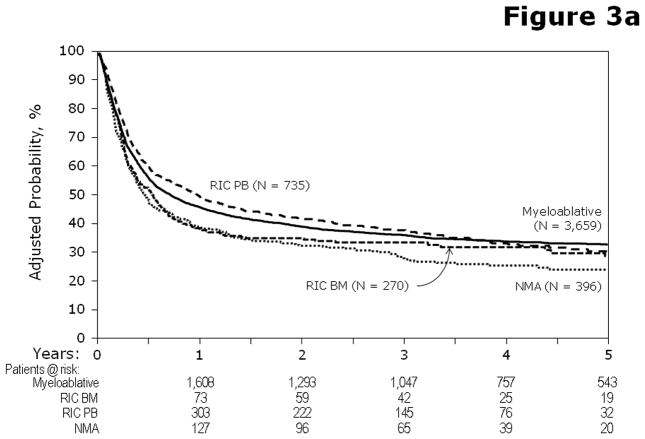
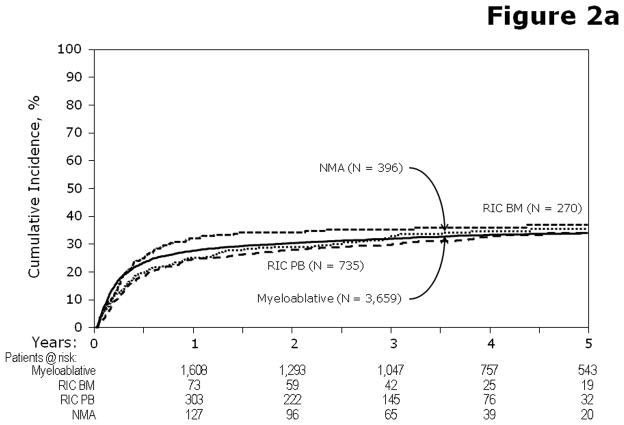
Although reduced-intensity conditioning (RIC) and non-myeloablative (NMA)-conditioning regimens have been used for over a decade, their relative efficacy vs myeloablative (MA) approaches to allogeneic hematopoietic cell transplantation in patients with AML and myelodysplasia (MDS) is unknown. We compared disease status, donor, graft and recipient characteristics with outcomes of 3731 MA with 1448 RIC/NMA procedures performed at 217 centers between 1997 and 2004. The 5-year univariate probabilities and multivariate relative risk outcomes of relapse, TRM, disease-free survival (DFS) and OS are reported. Adjusted OS at 5 years was 34, 33 and 26% for MA, RIC and NMA transplants, respectively. NMA conditioning resulted in inferior DFS and OS, but there was no difference in DFS and OS between RIC and MA regimens. Late TRM negates early decreases in toxicity with RIC and NMA regimens. Our data suggest that higher regimen intensity may contribute to optimal survival in patients with AML/MDS, suggesting roles for both regimen intensity and graft vs leukemia in these diseases. Prospective studies comparing regimens are needed to confirm this finding and determine the optimal approach to patients who are eligible for either MA or RIC/NMA conditioning.
虽然减强度预处理(RIC)和非清髓性(NMA)预处理方案已经应用了十余年,但其与清髓性(MA)预处理方案相比,在 AML 和骨髓增生异常综合征(MDS)患者中的异基因造血细胞移植中的相对疗效仍不清楚。我们比较了 1997 年至 2004 年间在 217 个中心接受 3731 例 MA 和 1448 例 RIC/NMA 治疗的患者的疾病状态、供者、移植物和受者特征与结局。报告了 5 年单变量概率和多变量相对风险的复发、TRM、无病生存(DFS)和总生存(OS)。5 年时,MA、RIC 和 NMA 移植的调整后 OS 分别为 34%、33%和 26%。NMA 预处理导致 DFS 和 OS 降低,但 RIC 和 MA 方案之间的 DFS 和 OS 没有差异。晚期 TRM 否定了 RIC 和 NMA 方案降低毒性的早期作用。我们的数据表明,更高的方案强度可能有助于 AML/MDS 患者获得最佳生存,这表明方案强度和移植物抗白血病在这些疾病中都有作用。需要进行前瞻性研究比较方案,以证实这一发现,并确定适合 MA 或 RIC/NMA 预处理的患者的最佳治疗方法。