Department of Hematology and Oncology, University of Regensburg Medical Center, Regensburg, Germany.
Bone Marrow Transplant. 2011 Oct;46(10):1283-95. doi: 10.1038/bmt.2011.35. Epub 2011 Mar 28.
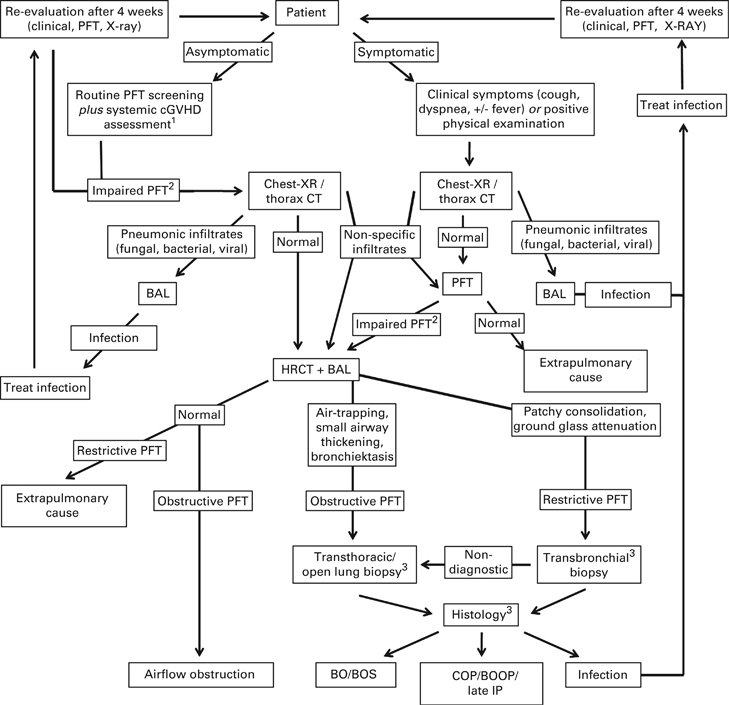
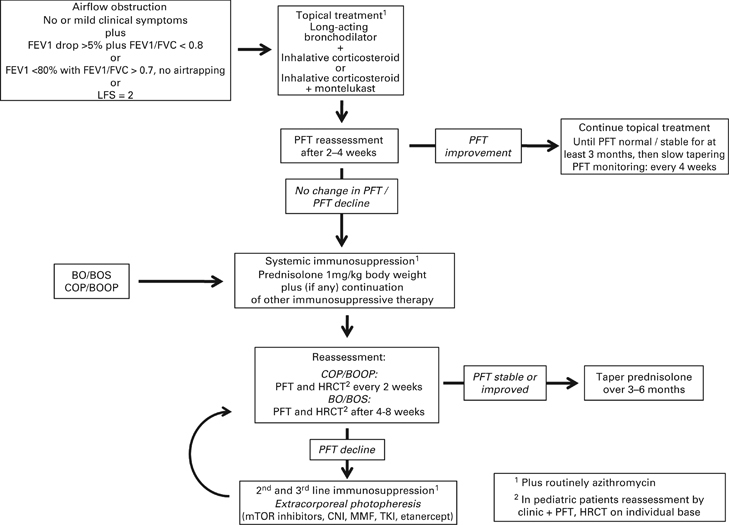
This consensus statement established under the auspices of the German working group on BM and blood stem cell transplantation (DAG-KBT), the German Society of Hematology and Oncology (DGHO), the Austrian Stem Cell Transplant Working Group, the Swiss Blood Stem Cell Transplantation Group (SBST) and the German-Austrian Pediatric Working Group on SCT (Päd-Ag-KBT) summarizes current evidence for diagnosis, immunosuppressive and supportive therapy to provide practical guidelines for the care and treatment of patients with pulmonary manifestations of chronic GVHD (cGVHD). Pulmonary cGVHD can present with obstructive and/or restrictive changes. Disease severity ranges from subclinical pulmonary function test (PFT) impairment to respiratory insufficiency with bronchiolitis obliterans being the only pulmonary complication currently considered diagnostic of cGVHD. Early diagnosis may improve clinical outcome, and regular post-transplant follow-up PFTs are recommended. Diagnostic work-up includes high-resolution computed tomography, bronchoalveolar lavage and histology. Topical treatment is based on inhalative steroids plus beta-agonists. Early addition of azithromycin is suggested. Systemic first-line treatment consists of corticosteroids plus, if any, continuation of other immunosuppressive therapy. Second-line therapy and beyond includes extracorporeal photopheresis, mammalian target of rapamycin inhibitors, mycophenolate, etanercept, imatinib and TLI, but efficacy is limited. Clinical trials are urgently needed to improve understanding and treatment of this deleterious complication.
本共识声明由德国骨髓和造血干细胞移植工作组(DAG-KBT)、德国血液学和肿瘤学会(DGHO)、奥地利造血干细胞移植工作组、瑞士造血干细胞移植组(SBST)和德国-奥地利儿科造血干细胞移植工作组(Päd-Ag-KBT)共同制定,总结了诊断、免疫抑制和支持治疗方面的最新证据,为慢性移植物抗宿主病(cGVHD)肺部表现患者的护理和治疗提供实用指南。肺部 cGVHD 可表现为阻塞性和/或限制性改变。疾病严重程度从亚临床肺功能测试(PFT)损害到呼吸功能不全不等,目前仅有细支气管炎性闭塞被认为是 cGVHD 的肺部并发症。早期诊断可能改善临床结局,建议进行定期移植后 PFT 随访。诊断工作包括高分辨率计算机断层扫描、支气管肺泡灌洗和组织学检查。局部治疗基于吸入性类固醇加β激动剂。建议早期加用阿奇霉素。一线系统治疗包括皮质类固醇加,如果有其他免疫抑制治疗,则继续使用。二线及以上治疗包括体外光化学疗法、雷帕霉素靶蛋白抑制剂、霉酚酸酯、依那西普、伊马替尼和 TLI,但疗效有限。迫切需要开展临床试验以改善对这种有害并发症的认识和治疗。