de Mulder M, van der Zant F M, Knaapen P, Cornel J H, Umans V A W M
Neth Heart J. 2011 Feb;19(2):68-72. doi: 10.1007/s12471-011-0075-7. Epub 2011 Feb 8.
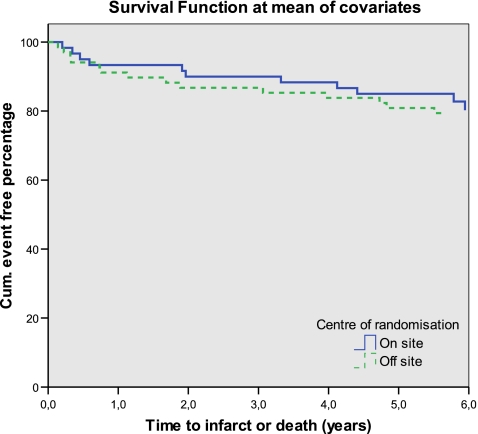
Primary percutaneous coronary intervention (PCI) is the preferred treatment option for acute myocardial infarction (MI). Off-site PCI reduces time-to-treatment, which could potentially lead to enhanced clinical outcomes. Therefore, we investigated whether off-site PCI improves 5-year clinical outcomes compared with on-site PCI and whether this is related to in-hospital (99m)Tc-sestamibi single photon emission computed tomography (MIBI SPECT) parameters. METHODS: We describe the 5-year follow-up for a combined endpoint of death or re-infarction in 128 patients with acute MI who were randomly assigned to undergo primary PCI at the off-site centre (n = 68) or to transferral to an on-site centre (n = 60). Three days after PCI, MIBI SPECT was performed to estimate infarct size. A multivariate Cox regression model was created to study the relation between MIBI SPECT parameters and long-term clinical outcomes. RESULTS: After a mean follow-up of 5.8 ± 1.1 years, 25 events occurred. Off-site PCI significantly reduced door-to-balloon time compared with on-site PCI (94 ± 54 versus 125 ± 59 min, p = 0.003). However, infarct size (17 ± 15 versus 14 ± 12%, p = 0.34) and 5-year death or infarct rate (21% versus 18%, p = 0.75) were comparable between treatment centres. With multivariate analysis, only Killip class ≥2 and Q wave MI, but not scintigraphic data, predicted long-term clinical outcomes. CONCLUSION: Off-site PCI reduced door-to-balloon time with a comparable 5-year death or infarct rate. Parameters from resting MIBI SPECT on day 3 after MI did not predict long-term clinical outcomes.
直接经皮冠状动脉介入治疗(PCI)是急性心肌梗死(MI)的首选治疗方案。非现场PCI可缩短治疗时间,这可能会改善临床结局。因此,我们研究了与现场PCI相比,非现场PCI是否能改善5年临床结局,以及这是否与住院期间的(99m)锝- sestamibi单光子发射计算机断层扫描(MIBI SPECT)参数有关。方法:我们描述了128例急性MI患者的5年随访情况,这些患者被随机分配到非现场中心接受直接PCI(n = 68)或转至现场中心(n = 60)。PCI术后3天,进行MIBI SPECT以评估梗死面积。建立多变量Cox回归模型来研究MIBI SPECT参数与长期临床结局之间的关系。结果:平均随访5.8±1.1年,发生了25起事件。与现场PCI相比,非现场PCI显著缩短了球囊扩张时间(94±54分钟对125±59分钟,p = 0.003)。然而,治疗中心之间的梗死面积(17±15%对14±12%,p = 0.34)和5年死亡率或梗死率(21%对18%,p = 0.75)相当。通过多变量分析,只有Killip分级≥2和Q波MI可预测长期临床结局,而闪烁扫描数据则不能。结论:非现场PCI缩短了球囊扩张时间,5年死亡率或梗死率相当。MI后第3天静息MIBI SPECT的参数不能预测长期临床结局。