Alberta Research Centre for Health Evidence, Department of Pediatrics, University of Alberta, 11402 University Avenue, Edmonton, AB, Canada T6G 2J3.
BMJ. 2011 Apr 6;342:d1714. doi: 10.1136/bmj.d1714.
To evaluate and compare the efficacy and safety of bronchodilators and steroids, alone or combined, for the acute management of bronchiolitis in children aged less than 2 years.
Systematic review and meta-analysis.
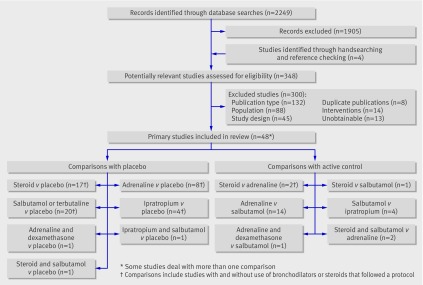
Medline, Embase, Central, Scopus, PubMed, LILACS, IranMedEx, conference proceedings, and trial registers. Inclusion criteria Randomised controlled trials of children aged 24 months or less with a first episode of bronchiolitis with wheezing comparing any bronchodilator or steroid, alone or combined, with placebo or another intervention (other bronchodilator, other steroid, standard care).
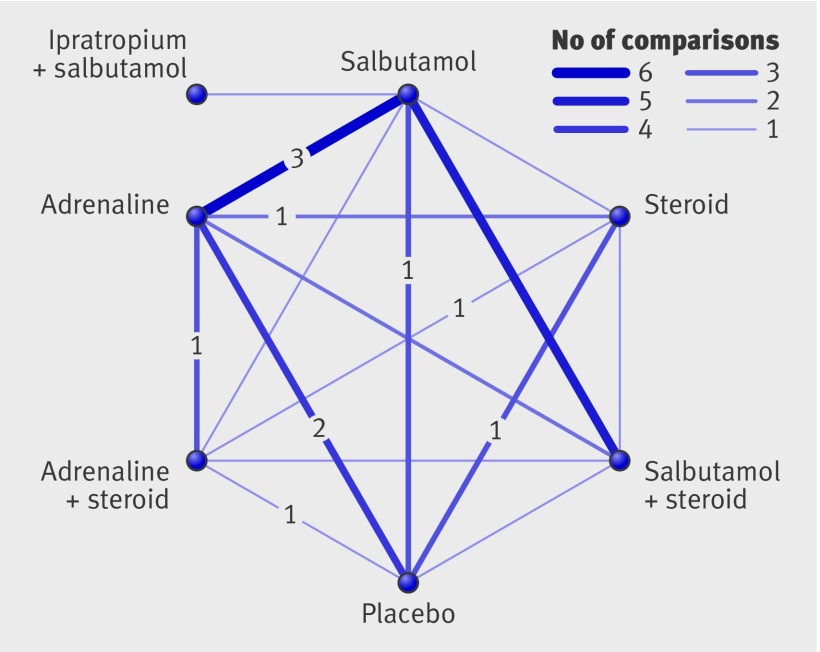
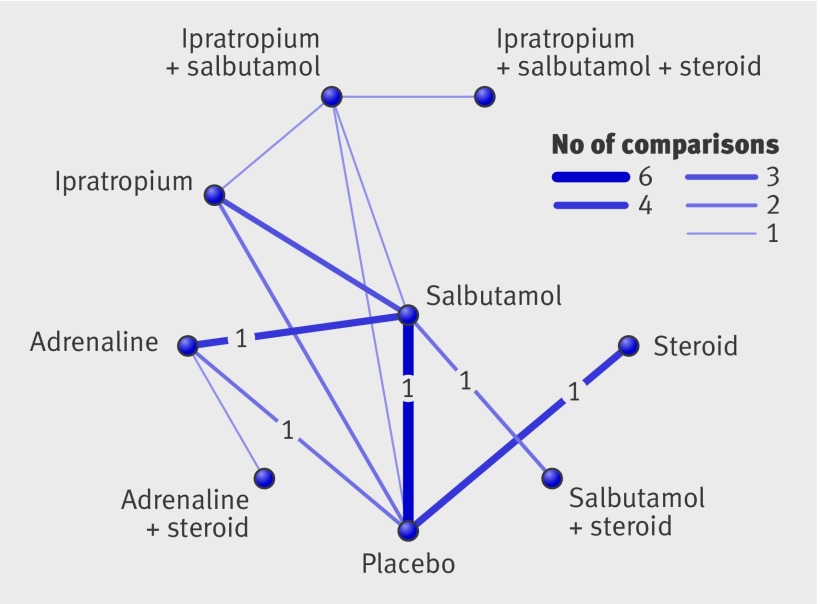
Two reviewers assessed studies for inclusion and risk of bias and extracted data. Primary outcomes were selected by clinicians a priori based on clinical relevance: rate of admission for outpatients (day 1 and up to day 7) and length of stay for inpatients. Direct meta-analyses were carried out using random effects models. A mixed treatment comparison using a Bayesian network model was used to compare all interventions simultaneously.
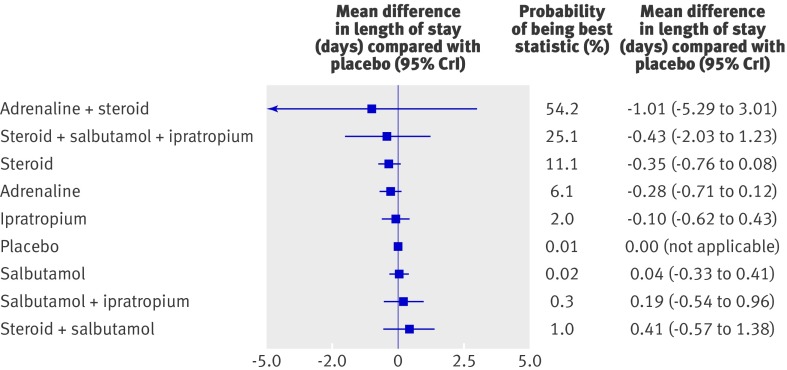
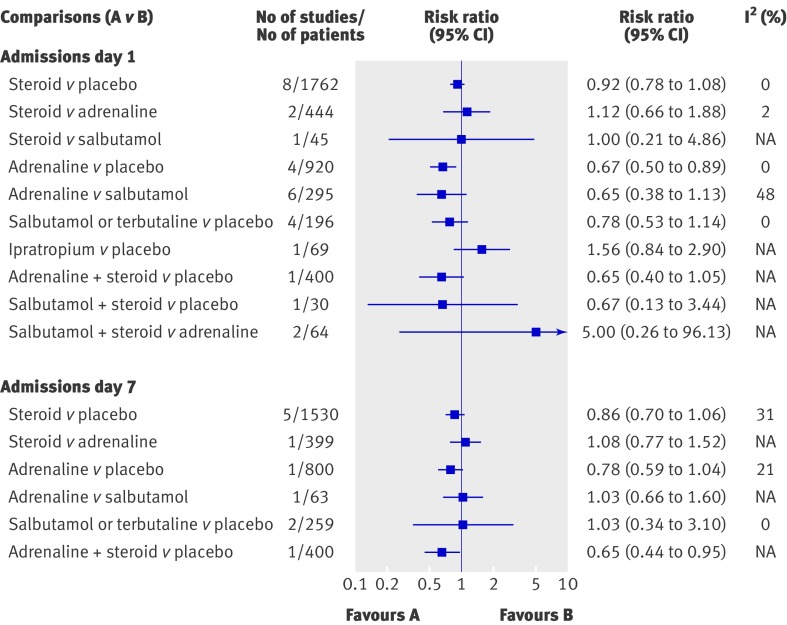
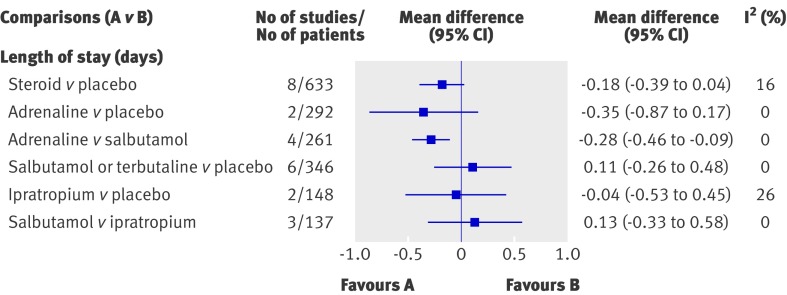
48 trials (4897 patients, 13 comparisons) were included. Risk of bias was low in 17% (n = 8), unclear in 52% (n = 25), and high in 31% (n = 15). Only adrenaline (epinephrine) reduced admissions on day 1 (compared with placebo: pooled risk ratio 0.67, 95% confidence interval 0.50 to 0.89; number needed to treat 15, 95% confidence interval 10 to 45 for a baseline risk of 20%; 920 patients). Unadjusted results from a single large trial with low risk of bias showed that combined dexamethasone and adrenaline reduced admissions on day 7 (risk ratio 0.65, 0.44 to 0.95; number needed to treat 11, 7 to 76 for a baseline risk of 26%; 400 patients). A mixed treatment comparison supported adrenaline alone or combined with steroids as the preferred treatments for outpatients (probability of being the best treatment based on admissions at day 1 were 45% and 39%, respectively). The incidence of reported harms did not differ. None of the interventions examined showed clear efficacy for length of stay among inpatients.
Evidence shows the effectiveness and superiority of adrenaline for outcomes of most clinical relevance among outpatients with acute bronchiolitis, and evidence from a single precise trial for combined adrenaline and dexamethasone.
评估和比较单独或联合使用支气管扩张剂和类固醇治疗 2 岁以下儿童毛细支气管炎的疗效和安全性。
系统评价和荟萃分析。
Medline、Embase、Central、Scopus、PubMed、LILACS、IranMedEx、会议记录和试验登记处。纳入标准:年龄 24 个月或以下,首次出现喘息性毛细支气管炎的儿童,随机对照试验,比较任何支气管扩张剂或类固醇,单独或联合,与安慰剂或其他干预(其他支气管扩张剂、其他类固醇、标准治疗)。
两名评审员评估研究的纳入和偏倚风险,并提取数据。主要结局由临床医生根据临床相关性预先选择:门诊患者的入院率(第 1 天和第 7 天)和住院患者的住院时间。直接荟萃分析采用随机效应模型进行。使用贝叶斯网络模型进行混合治疗比较,以同时比较所有干预措施。
共纳入 48 项试验(4897 例患者,13 项比较)。17%(n=8)的试验风险低,52%(n=25)的试验风险不确定,31%(n=15)的试验风险高。只有肾上腺素(epinephrine)可降低第 1 天的入院率(与安慰剂相比:汇总风险比 0.67,95%置信区间 0.50 至 0.89;需要治疗的人数 15,95%置信区间 10 至 45,基线风险为 20%;920 例患者)。一项风险低的单一大规模试验的未调整结果显示,联合使用地塞米松和肾上腺素可降低第 7 天的入院率(风险比 0.65,0.44 至 0.95;需要治疗的人数 11,7 至 76,基线风险为 26%;400 例患者)。一项混合治疗比较支持单独使用肾上腺素或联合使用类固醇作为门诊患者的首选治疗方法(基于第 1 天入院率,分别为 45%和 39%的最佳治疗可能性)。报告的不良反应发生率没有差异。在住院患者中,没有一种干预措施在住院时间方面显示出明显的疗效。
有证据表明,肾上腺素在急性毛细支气管炎门诊患者中对大多数临床相关结局具有有效性和优越性,并且一项单一大规模精确试验表明肾上腺素联合地塞米松具有优越性。