Walid M Sami, Robinson Joe Sam, Abbara Moataz, Tolaymat Abdullah, Robinson Joe Sam
Georgia NeuroCenter, Medical Center of Central Georgia, Macon, GA, USA.
Ger Med Sci. 2011 Apr 21;9:Doc10. doi: 10.3205/000133.
Degenerative spine disorders are steadily increasing parallel to the aging of the population with considerable impact on cost and productivity. In this paper we study the prevalence and risk factors for multiple spine surgery and its impact on cost.
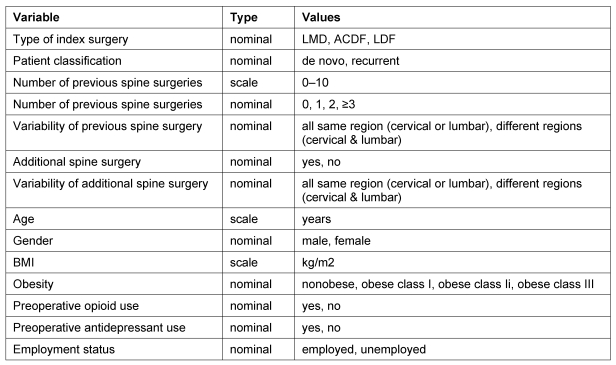
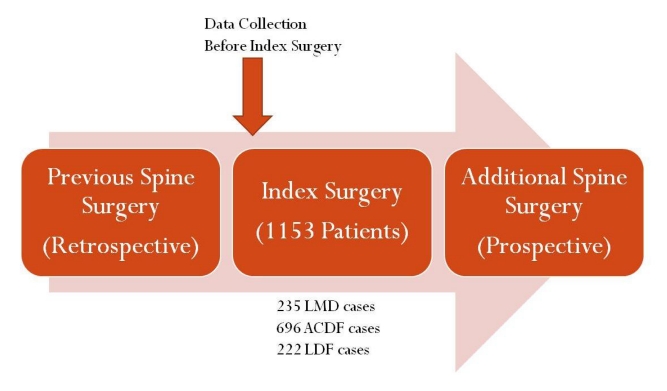
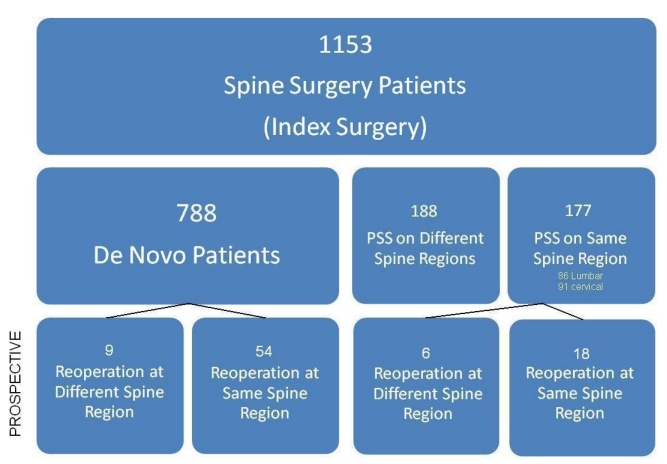
Data on 1,153 spine surgery inpatients operated between October 2005 and September 2008 (index spine surgery) in regard to the number of previous spine surgeries and location of surgeries (cervical or lumbar) were retrospectively collected. Additionally, prospective follow-up over a period of 2-5 years was conducted.
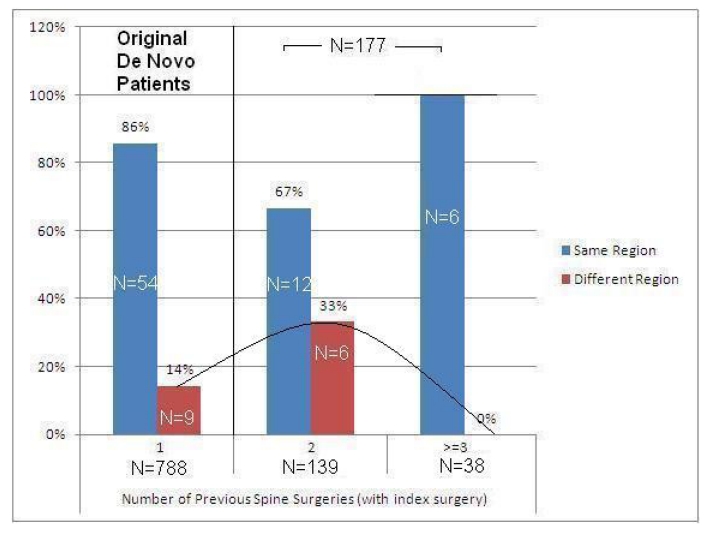
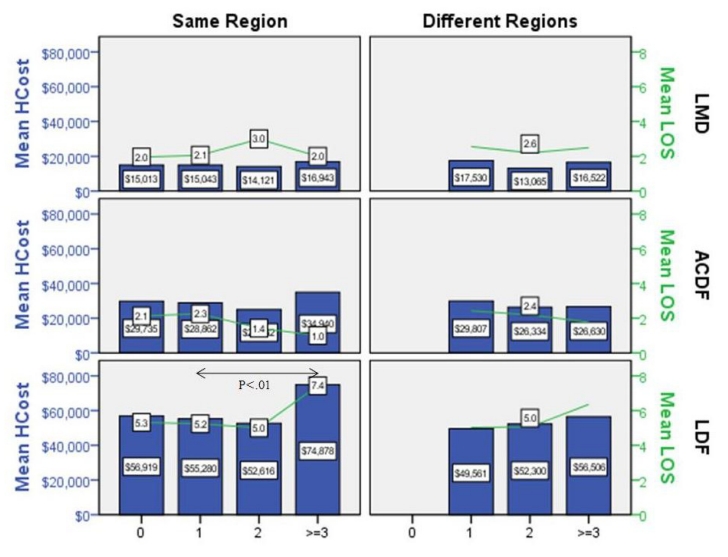
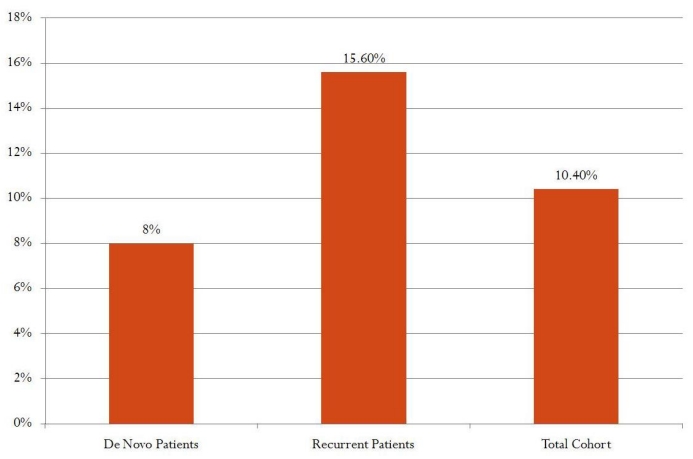
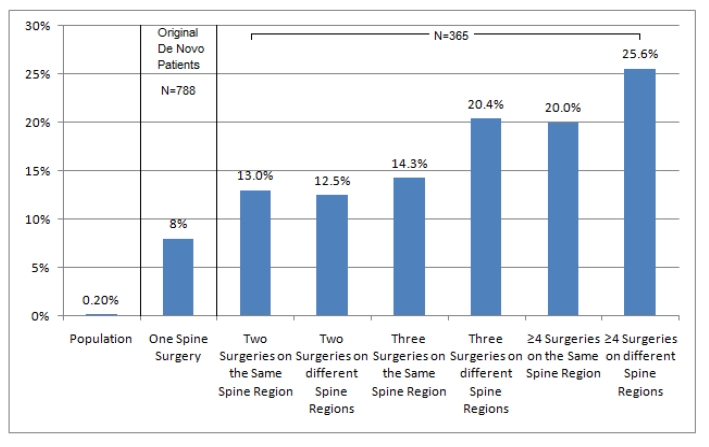
Retrospectively, 365 (31.7%) patients were recurrent spine surgery patients while 788 (68.3%) were de novo spine surgery patients.Nearly half of those with previous spine surgery (51.5%) were on different regions of the spine. There were no significant differences in length of stay or hospital charges except in lumbar decompression and fusion (LDF) patients with multiple interventions on the same region of the spine. Significant differences (P<.05) in length of stay (5.4 days vs. 7.4 days) and hospital charges ($55,477 vs. $74,878) between LDF patients with one previous spine versus those with ≥3 previous spine surgeries on the same region were noted.Prospectively, the overall reoperation rate was 10.4%. The risk of additional spine surgery increased from 8.0% in patients with one previous spine surgery (index surgery) to 25.6% in patients with ≥4 previous spine surgeries on different regions of the spine (including index surgery).After excluding patients with previous spine surgeries on different regions of the spine, 17.2% of reoperated patients had additional spine surgery on a different spine region. The percentage of additional spine surgery on a distant spine region increased from 14.0% in patients with one spine surgery to 33.0% in patients with two spine surgeries on the same region. However, in patients with three or more spine surgeries on the same spine region there were no interventions on a distant spine region during the follow-up period.
De novo spine surgery is associated with an increased incidence of additional spine surgery at the same or distant spine regions. Large prospective studies with extended follow-up periods and multifaceted cost-outcome analysis are needed to refine the appropriateness of spine surgery.
随着人口老龄化,退行性脊柱疾病呈稳步上升趋势,对成本和生产力产生了重大影响。在本文中,我们研究了多次脊柱手术的患病率、风险因素及其对成本的影响。
回顾性收集了2005年10月至2008年9月期间接受手术的1153例脊柱手术住院患者(索引脊柱手术)的既往脊柱手术次数和手术部位(颈椎或腰椎)的数据。此外,还进行了为期2至5年的前瞻性随访。
回顾性分析显示,365例(31.7%)患者为复发性脊柱手术患者,788例(68.3%)为初次脊柱手术患者。近一半曾接受过脊柱手术的患者(51.5%)手术部位位于脊柱的不同区域。除了在同一脊柱区域接受多次干预的腰椎减压融合术(LDF)患者外,住院时间和住院费用没有显著差异。在同一区域接受过一次脊柱手术的LDF患者与接受过≥3次脊柱手术的患者之间,住院时间(5.4天对7.4天)和住院费用(55477美元对74878美元)存在显著差异(P<0.05)。前瞻性分析显示,总体再次手术率为10.4%。脊柱再次手术的风险从接受过一次脊柱手术(索引手术)的患者的8.0%增加到在脊柱不同区域接受过≥4次脊柱手术(包括索引手术)的患者的25.6%。排除在脊柱不同区域接受过既往脊柱手术的患者后,17.2%的再次手术患者在不同脊柱区域进行了额外的脊柱手术。在同一区域接受一次脊柱手术的患者中,在远处脊柱区域进行额外脊柱手术的比例从14.0%增加到接受两次脊柱手术的患者的33.0%。然而,在同一脊柱区域接受过三次或更多次脊柱手术的患者在随访期间没有在远处脊柱区域进行干预。
初次脊柱手术与在同一或远处脊柱区域进行额外脊柱手术的发生率增加相关。需要进行长期随访的大型前瞻性研究和多方面的成本效益分析,以完善脊柱手术的合理性。