Division of Rheumatology, Department of Medicine, University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School, New Brunswick, USA.
Ann Rheum Dis. 2011 Jul;70(7):1264-71. doi: 10.1136/ard.2010.144063. Epub 2011 May 3.
This study assessed the efficacy and safety of canakinumab, a fully human anti-interleukin 1β monoclonal antibody, for prophylaxis against acute gouty arthritis flares in patients initiating urate-lowering treatment.
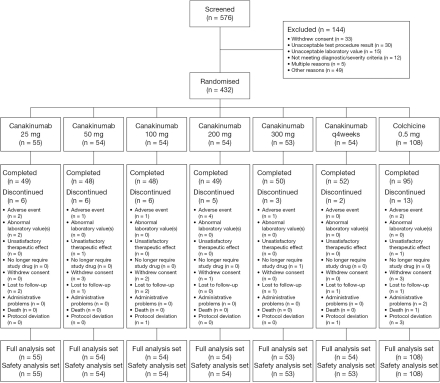
In this double-blind, double-dummy, dose-ranging study, 432 patients with gouty arthritis initiating allopurinol treatment were randomised 1:1:1:1:1:1:2 to receive: a single dose of canakinumab, 25, 50, 100, 200, or 300 mg subcutaneously; 4×4-weekly doses of canakinumab (50+50+25+25 mg subcutaneously); or daily colchicine 0.5 mg orally for 16 weeks. Patients recorded details of flares in diaries. The study aimed to determine the canakinumab dose having equivalent efficacy to colchicine 0.5 mg at 16 weeks.
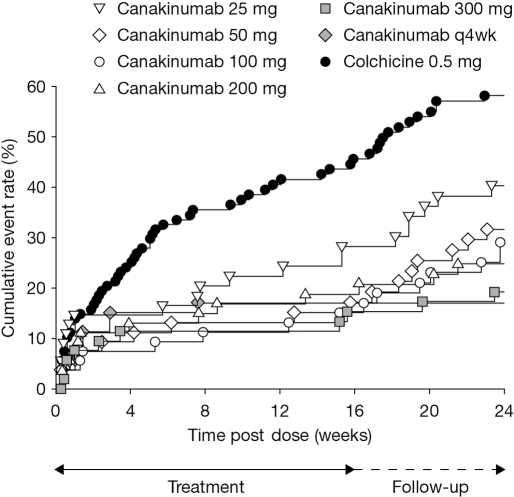
A dose-response for canakinumab was not apparent with any of the four predefined dose-response models. The estimated canakinumab dose with equivalent efficacy to colchicine was below the range of doses tested. At 16 weeks, there was a 62% to 72% reduction in the mean number of flares per patient for canakinumab doses ≥50 mg versus colchicine based on a negative binomial model (rate ratio: 0.28-0.38, p≤0.0083), and the percentage of patients experiencing ≥1 flare was significantly lower for all canakinumab doses (15% to 27%) versus colchicine (44%, p<0.05). There was a 64% to 72% reduction in the risk of experiencing ≥1 flare for canakinumab doses ≥50 mg versus colchicine at 16 weeks (hazard ratio (HR): 0.28-0.36, p≤0.05). The incidence of adverse events was similar across treatment groups.
Single canakinumab doses ≥50 mg or four 4-weekly doses provided superior prophylaxis against flares compared with daily colchicine 0.5 mg.
本研究评估了完全人源抗白细胞介素 1β 单克隆抗体卡那单抗预防开始尿酸降低治疗的痛风性关节炎急性发作的疗效和安全性。
在这项双盲、双模拟、剂量范围研究中,432 例开始别嘌醇治疗的痛风性关节炎患者按 1:1:1:1:1:1:2 随机分组,接受:单次皮下注射卡那单抗 25、50、100、200 或 300mg;4×4 周剂量的卡那单抗(50+50+25+25mg 皮下注射);或每日口服秋水仙碱 0.5mg,共 16 周。患者在日记中记录发作详情。该研究旨在确定卡那单抗剂量与 16 周时秋水仙碱 0.5mg 等效的疗效。
在任何四个预设的剂量反应模型中,都没有出现卡那单抗的剂量反应。估计与秋水仙碱等效的卡那单抗剂量低于测试剂量范围。在 16 周时,基于负二项式模型,与秋水仙碱相比,卡那单抗剂量≥50mg 的患者平均发作次数减少了 62%至 72%(率比:0.28-0.38,p≤0.0083),并且所有卡那单抗剂量(15%至 27%)的患者经历≥1 次发作的百分比明显低于秋水仙碱(44%,p<0.05)。与秋水仙碱相比,在 16 周时,卡那单抗剂量≥50mg 降低了≥1 次发作的风险 64%至 72%(风险比(HR):0.28-0.36,p≤0.05)。各组不良反应发生率相似。
单次卡那单抗剂量≥50mg 或 4 个 4 周剂量与每日秋水仙碱 0.5mg 相比,能更有效地预防发作。