University of Sheffield School of Clinical Dentistry, Sheffield S10 2TA, UK.
BMJ. 2011 May 3;342:d2392. doi: 10.1136/bmj.d2392.
To quantify the change in prescribing of antibiotic prophylaxis before invasive dental procedures for patients at risk of infective endocarditis, and any concurrent change in the incidence of infective endocarditis, following introduction of a clinical guideline from the National Institute for Health and Clinical Excellence (NICE) in March 2008 recommending the cessation of antibiotic prophylaxis in the United Kingdom.
Before and after study.
England. Population All patients admitted to hospital in England with a primary or secondary discharge diagnosis of acute or subacute infective endocarditis.
Monthly number of prescriptions for antibiotic prophylaxis consisting of a single 3 g oral dose of amoxicillin or a single 600 mg oral dose of clindamycin, and monthly number of cases of infective endocarditis, infective endocarditis related deaths in hospital, or cases of infective endocarditis with a possible oral origin for streptococci.
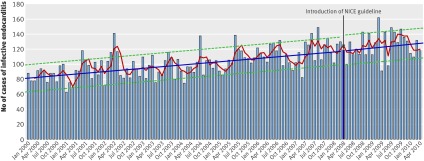
After the introduction of the NICE guideline there was a highly significant 78.6% reduction (P < 0.001) in prescribing of antibiotic prophylaxis, from a mean 10,277 (SD 1068) prescriptions per month to 2292 (SD 176). Evidence that the general upward trend in cases of infective endocarditis before the guideline was significantly altered after the guideline was lacking (P = 0.61). Using a non-inferiority test, an increase in the number of cases of 9.3% or more could be excluded after the introduction of the guideline. Similarly an increase in infective endocarditis related deaths in hospital of 12.3% or more could also be excluded.
Despite a 78.6% reduction in prescribing of antibiotic prophylaxis after the introduction of the NICE guideline, this study excluded any large increase in the incidence of cases of or deaths from infective endocarditis in the two years after the guideline. Although this lends support to the guideline, ongoing data monitoring is needed to confirm this, and further clinical trials should determine if antibiotic prophylaxis still has a role in protecting some patients at particularly high risk.
量化 2008 年 3 月英国国家健康与临床优化研究所(NICE)发布的临床指南建议停止在英国使用抗生素预防后,接受侵入性牙科手术的感染性心内膜炎高危患者的抗生素预防处方变化情况,以及感染性心内膜炎的发病率是否有任何变化。
前后研究。
英格兰。人群所有在英格兰住院的患者,其主要或次要出院诊断为急性或亚急性感染性心内膜炎。
每月开具的抗生素预防处方数量,包括单次 3 克口服阿莫西林或单次 600 毫克口服克林霉素,以及每月感染性心内膜炎、感染性心内膜炎相关院内死亡或可能由链球菌引起的感染性心内膜炎病例数。
在 NICE 指南发布后,抗生素预防处方显著减少了 78.6%(P<0.001),从每月平均 10277(SD 1068)张处方减少至 2292(SD 176)张。在指南发布前,感染性心内膜炎病例呈总体上升趋势,而在指南发布后,这种趋势明显改变的证据并不充分(P=0.61)。采用非劣效性检验,可排除指南发布后病例数增加 9.3%或更多的可能性。同样,可排除院内感染性心内膜炎相关死亡人数增加 12.3%或更多的可能性。
尽管在 NICE 指南发布后,抗生素预防处方减少了 78.6%,但本研究排除了指南发布后两年内感染性心内膜炎病例或死亡人数增加的可能性。尽管这为指南提供了支持,但仍需要进行持续的数据监测以确认这一点,并且需要进一步的临床试验来确定抗生素预防是否仍然对某些高危患者具有保护作用。