Masi Alfonse T, Nair Kalyani, Evans Tyler, Ghandour Yousef
Departments of Medicine and Epidemiology, University of Illinois, College of Medicine at Peoria, Peoria, IL;
Int J Ther Massage Bodywork. 2010 Dec 16;3(4):16-28. doi: 10.3822/ijtmb.v3i4.104.
Myofascial tissues generate integrated webs and networks of passive and active tensional forces that provide stabilizing support and that control movement in the body. Passive [central nervous system (CNS)-independent] resting myofascial tension is present in the body and provides a low-level stabilizing component to help maintain balanced postures. This property was recently called "human resting myofascial tone" (HRMT). The HRMT model evolved from electromyography (EMG) research in the 1950s that showed lumbar muscles usually to be EMG-silent in relaxed gravity-neutral upright postures.
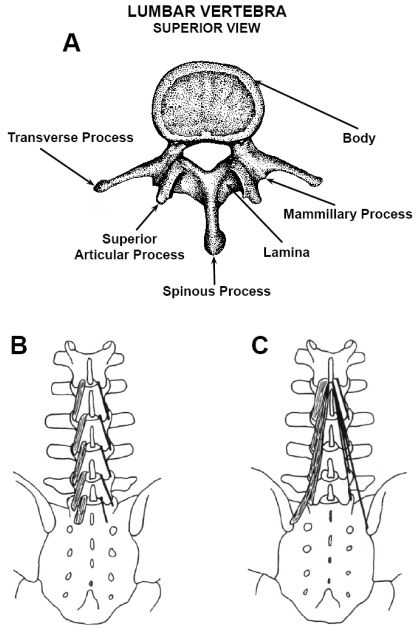
Biomechanical, clinical, and physiological studies were reviewed to interpret the passive stiffness properties of HRMT that help to stabilize various relaxed functions such as quiet balanced standing. Biomechanical analyses and experimental studies of the lumbar multifidus were reviewed to interpret its passive stiffness properties. The lumbar multifidus was illustrated as the major core stabilizing muscle of the spine, serving an important passive biomechanical role in the body.
Research into muscle physiology suggests that passive resting tension (CNS-independent) is generated in sarcomeres by the molecular elasticity of low-level cycling cross-bridges between the actomyosin filaments. In turn, tension is complexly transmitted to intimately enveloping fascial matrix fibrils and other molecular elements in connective tissue, which, collectively, constitute the myofascial unit. Postural myofascial tonus varies with age and sex. Also, individuals in the population are proposed to vary in a polymorphism of postural HRMT. A few people are expected to have outlier degrees of innate postural hypotonicity or hypertonicity. Such biomechanical variations likely predispose to greater risk of related musculoskeletal disorders, a situation that deserves greater attention in clinical practice and research. Axial myofascial hypertonicity was hypothesized to predispose to ankylosing spondylitis. This often-progressive deforming condition of vertebrae and sacroiliac joints is characterized by stiffness features and particular localization of bony lesions at entheseal sites. Such unique features imply concentrations and transmissions of excessive force, leading to tissue micro-injury and maladaptive repair reactions.
The HRMT model is now expanded and translated for clinical relevance to therapists. Its passive role in helping to maintain balanced postures is supported by biomechanical principles of myofascial elasticity, tension, stress, stiffness, and tensegrity. Further research is needed to determine the molecular basis of HRMT in sarcomeres, the transmission of tension by the enveloping fascial elements, and the means by which the myofascia helps to maintain efficient passive postural balance in the body. Significant deficiencies or excesses of postural HRMT may predispose to symptomatic or pathologic musculoskeletal disorders whose mechanisms are currently unexplained.
肌筋膜组织产生被动和主动张力的整合网络,为身体提供稳定支撑并控制运动。被动[独立于中枢神经系统(CNS)]的静息肌筋膜张力存在于体内,为维持平衡姿势提供低水平的稳定成分。这一特性最近被称为“人体静息肌筋膜张力”(HRMT)。HRMT模型源于20世纪50年代的肌电图(EMG)研究,该研究表明,在放松的重力中立直立姿势下,腰部肌肉通常处于EMG静息状态。
回顾生物力学、临床和生理学研究,以解释HRMT的被动僵硬度特性,这些特性有助于稳定各种放松功能,如安静的平衡站立。回顾了腰椎多裂肌的生物力学分析和实验研究,以解释其被动僵硬度特性。腰椎多裂肌被视为脊柱的主要核心稳定肌肉,在身体中发挥重要的被动生物力学作用。
肌肉生理学研究表明,被动静息张力(独立于CNS)由肌动球蛋白丝之间低水平循环横桥的分子弹性在肌节中产生。反过来,张力被复杂地传递到紧密包裹的筋膜基质纤维和结缔组织中的其他分子成分,这些成分共同构成肌筋膜单元。姿势性肌筋膜张力随年龄和性别而变化。此外,人群中的个体在姿势性HRMT的多态性方面也存在差异。预计少数人会有先天性姿势性张力过低或过高的异常程度。这种生物力学变化可能使相关肌肉骨骼疾病风险增加,这种情况在临床实践和研究中值得更多关注。轴向肌筋膜张力过高被假设易患强直性脊柱炎。这种通常进行性的椎骨和骶髂关节变形疾病的特征是僵硬特征以及骨病变在附着点部位的特定定位。这些独特特征意味着过度力的集中和传递,导致组织微损伤和适应性不良的修复反应。
HRMT模型现已扩展并转化为与治疗师临床相关的内容。其在帮助维持平衡姿势方面的被动作用得到了肌筋膜弹性、张力、应力、僵硬度和张拉整体结构生物力学原理的支持。需要进一步研究以确定肌节中HRMT的分子基础、包裹性筋膜元件对张力的传递以及肌筋膜帮助身体维持有效被动姿势平衡的方式。姿势性HRMT的显著不足或过度可能易患目前机制不明的有症状或病理性肌肉骨骼疾病。