University of Wisconsin School of Medicine and Public Health, Madison, WI 53792-3252, USA.
J Bone Miner Res. 2011 Sep;26(9):2194-203. doi: 10.1002/jbmr.428.
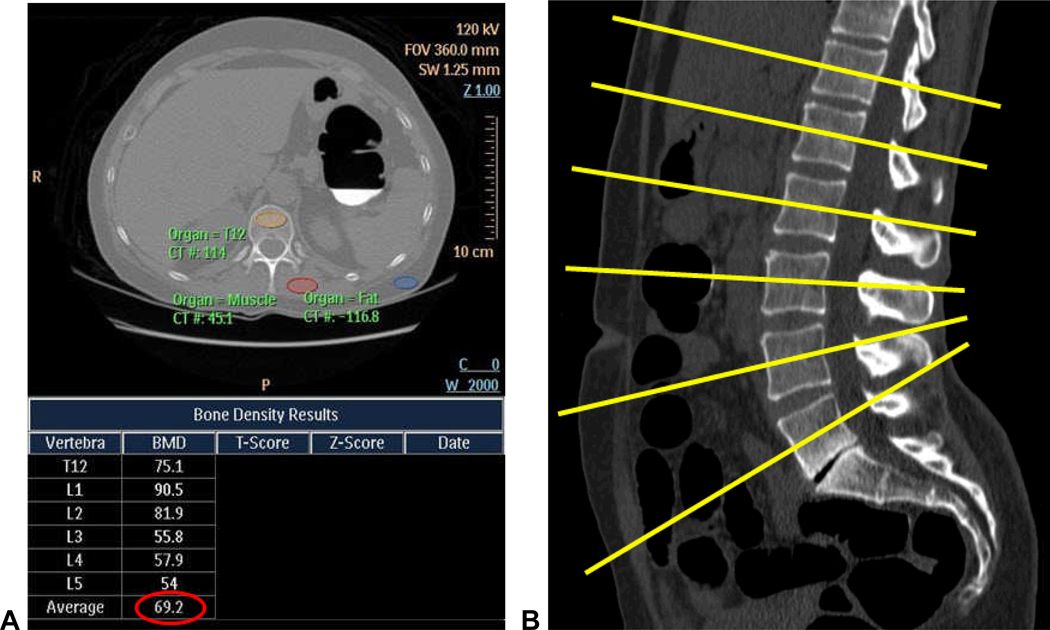
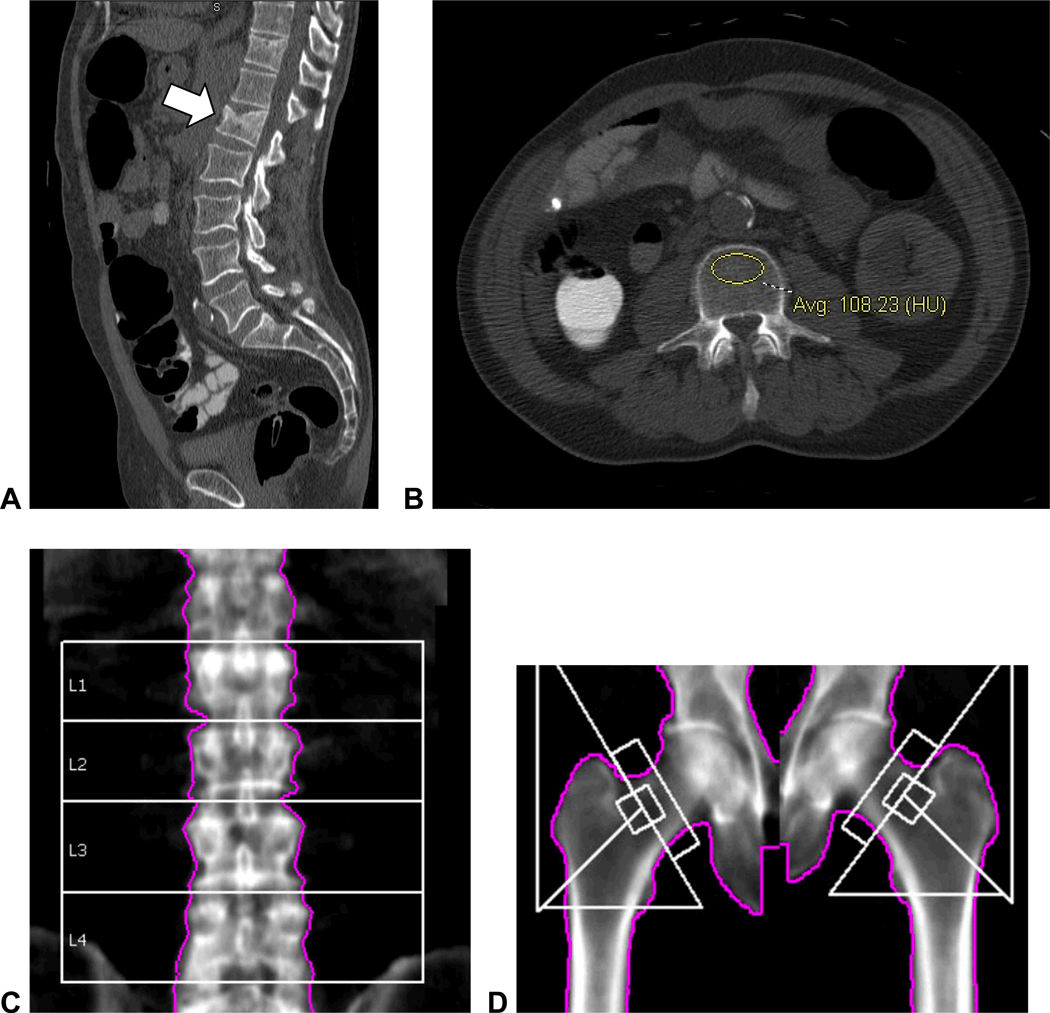
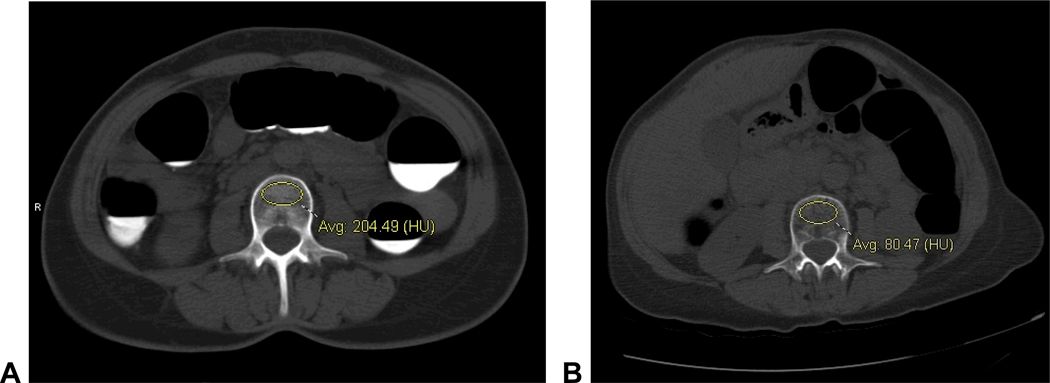
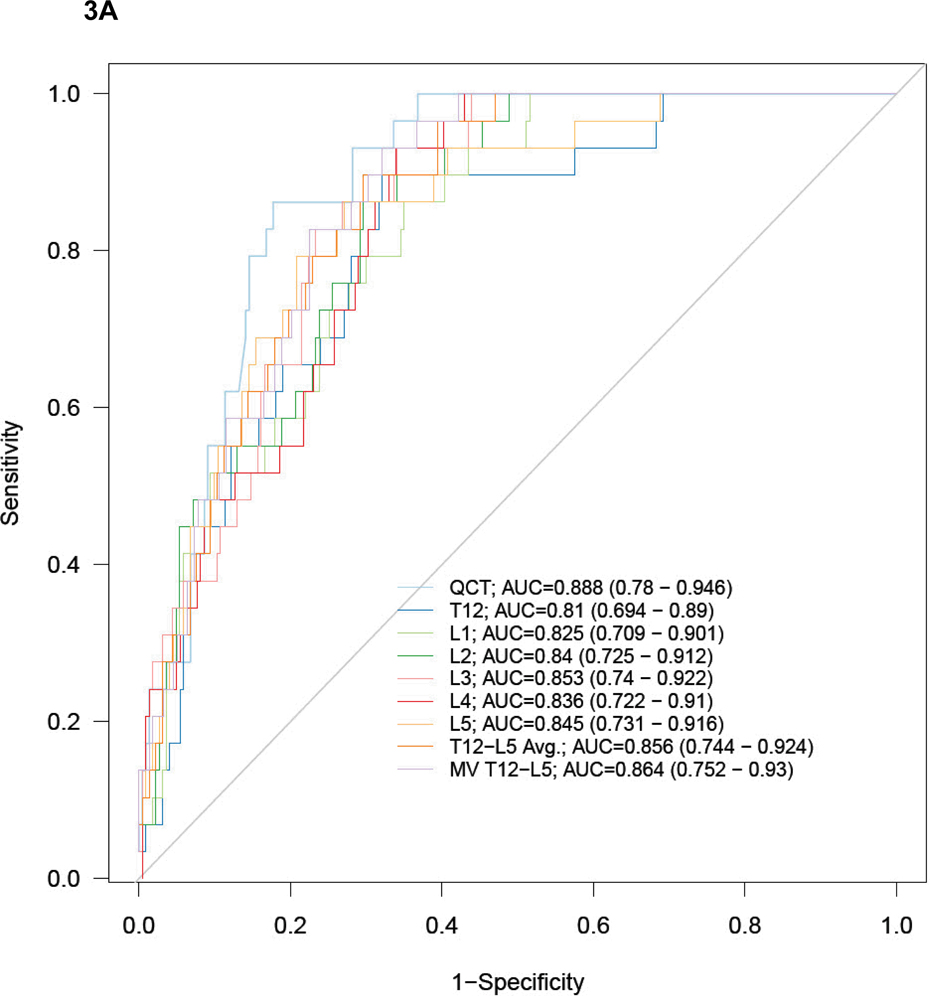
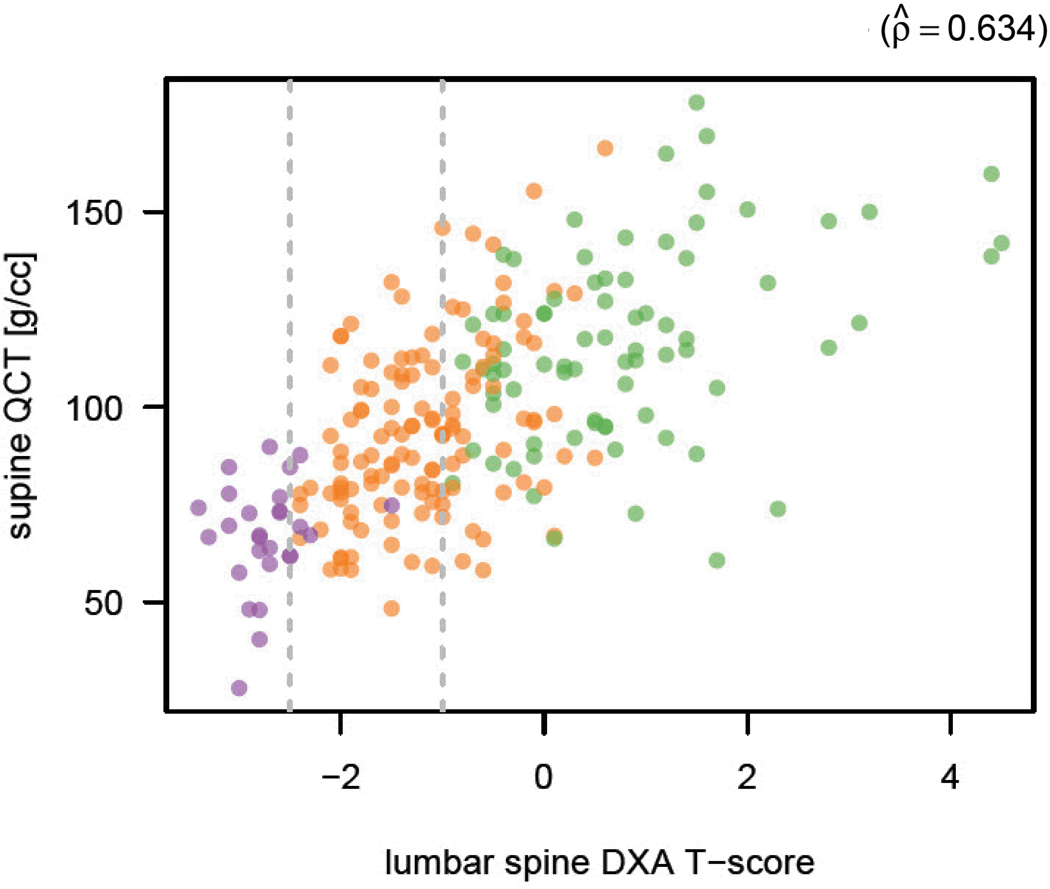
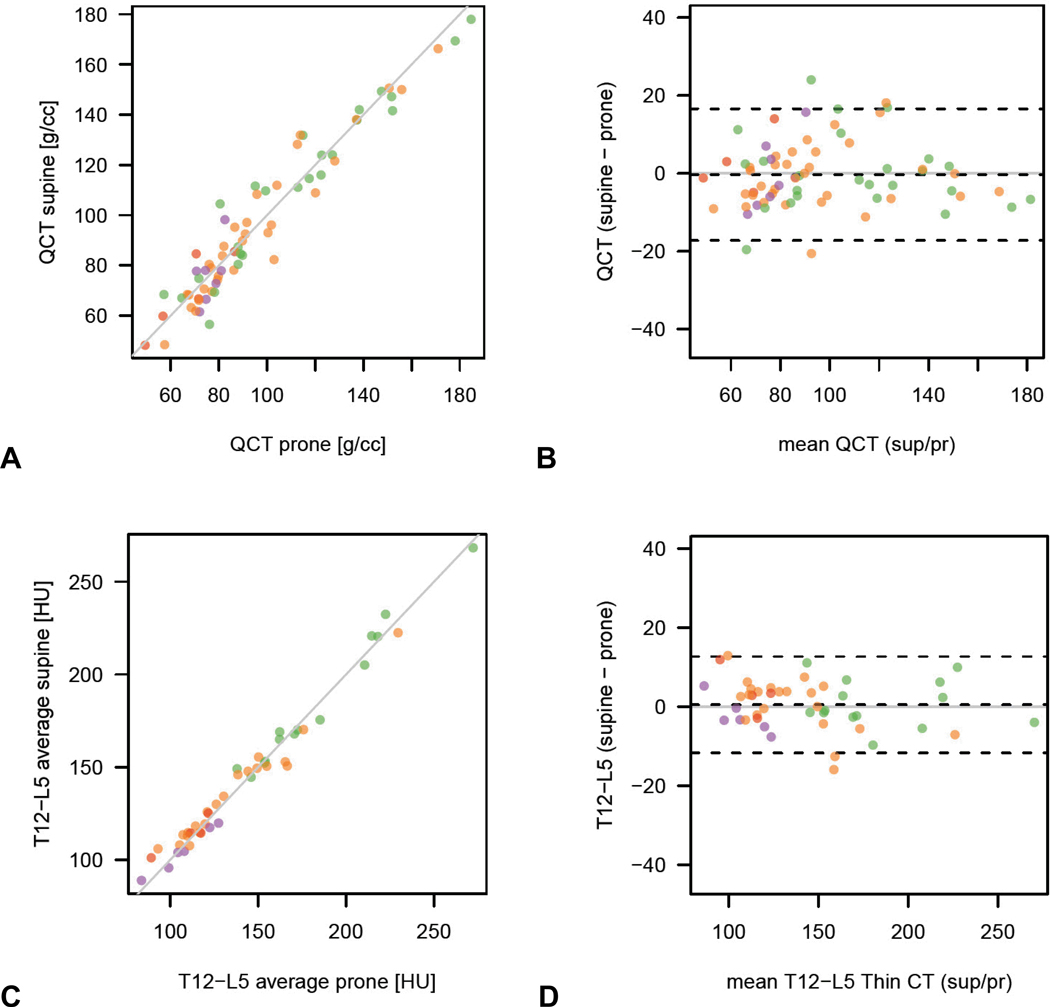
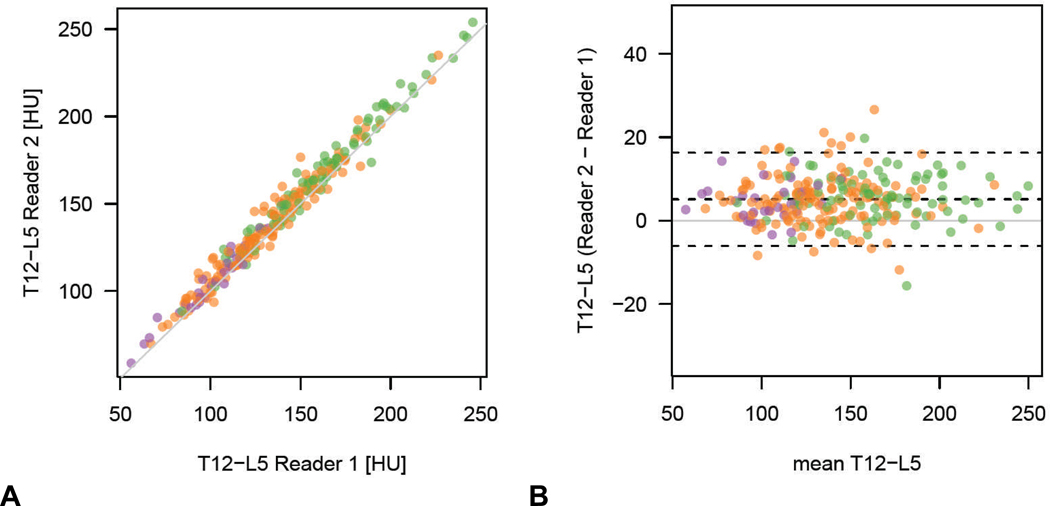
The purpose of this study was to evaluate the utility of lumbar spine attenuation measurement for bone mineral density (BMD) assessment at screening computed tomographic colonography (CTC) using central dual-energy X-ray absorptiometry (DXA) as the reference standard. Two-hundred and fifty-two adults (240 women and 12 men; mean age 58.9 years) underwent CTC screening and central DXA BMD measurement within 2 months (mean interval 25.0 days). The lowest DXA T-score between the spine and hip served as the reference standard, with low BMD defined per World Health Organization as osteoporosis (DXA T-score ≤ -2.5) or osteopenia (DXA T-score between -1.0 and -2.4). Both phantomless quantitative computed tomography (QCT) and simple nonangled region-of-interest (ROI) multi-detector CT (MDCT) attenuation measurements were applied to the T(12) -L(5) levels. The ability to predict osteoporosis and low BMD (osteoporosis or osteopenia) by DXA was assessed. A BMD cut-off of 90 mg/mL at phantomless QCT yielded 100% sensitivity for osteoporosis (29 of 29) and a specificity of 63.8% (143 of 224); 87.2% (96 of 110) below this threshold had low BMD and 49.6% (69 of 139) above this threshold had normal BMD at DXA. At L(1) , a trabecular ROI attenuation cut-off of 160 HU was 100% sensitive for osteoporosis (29 of 29), with a specificity of 46.4% (104 of 224); 83.9% (125 of 149) below this threshold had low BMD and 57.5% (59/103) above had normal BMD at DXA. ROI performance was similar at all individual T(12) -L(5) levels. At ROC analysis, AUC for osteoporosis was 0.888 for phantomless QCT [95% confidence interval (CI) 0.780-0.946] and ranged from 0.825 to 0.853 using trabecular ROIs at single lumbar levels (0.864; 95% CI 0.752-0.930 at multivariate analysis). Supine-prone reproducibility was better with the simple ROI method compared with QCT. It is concluded that both phantomless QCT and simple ROI attenuation measurements of the lumbar spine are effective for BMD screening at CTC with high sensitivity for osteoporosis, as defined by the DXA T-score.
本研究旨在评估腰椎衰减测量在使用中央双能 X 射线吸收法(DXA)作为参考标准的筛查性计算机断层结肠造影术(CTC)中的骨密度(BMD)评估中的效用。252 名成年人(240 名女性和 12 名男性;平均年龄 58.9 岁)在 2 个月内接受 CTC 筛查和中央 DXA BMD 测量(平均间隔 25.0 天)。最低的 DXA T 评分(脊柱和臀部之间)用作参考标准,根据世界卫生组织的定义,低 BMD 为骨质疏松症(DXA T 评分≤-2.5)或骨量减少症(DXA T 评分在-1.0 至-2.4 之间)。均采用无伪影定量 CT(QCT)和简单非角度感兴趣区(ROI)多探测器 CT(MDCT)衰减测量法对 T(12)-L(5)水平进行评估。评估了 DXA 预测骨质疏松症和低 BMD(骨质疏松症或骨量减少症)的能力。无伪影 QCT 中 BMD 截断值为 90mg/mL 时,对骨质疏松症的敏感性为 100%(29/29),特异性为 63.8%(143/224);低于此阈值的 87.2%(110/125)有低 BMD,高于此阈值的 49.6%(139/279)在 DXA 中有正常的 BMD。在 L(1),骨小梁 ROI 衰减截断值为 160HU 时,对骨质疏松症的敏感性为 100%(29/29),特异性为 46.4%(104/224);低于此阈值的 83.9%(149/178)有低 BMD,高于此阈值的 57.5%(103/181)在 DXA 中有正常的 BMD。ROI 性能在所有单独的 T(12)-L(5)水平上均相似。在 ROC 分析中,无伪影 QCT 的骨质疏松症 AUC 为 0.888(95%置信区间[CI]为 0.780-0.946),在单个腰椎水平使用骨小梁 ROI 时范围为 0.825 至 0.853(0.864;95%CI 为 0.752-0.930 在多变量分析中)。与 QCT 相比,仰卧位-俯卧位重复性更好。结论是,无伪影 QCT 和腰椎简单 ROI 衰减测量均能有效筛查 CTC 的 BMD,对骨质疏松症具有较高的敏感性,其定义为 DXA T 评分。