Dept. of Radiation, Oncology INF, Heidelberg Germany.
BMC Cancer. 2011 May 19;11:182. doi: 10.1186/1471-2407-11-182.
Long-term locoregional control in locally advanced squamous cell carcinoma of the head and neck (SCCHN) remains challenging. While recent years have seen various approaches to improve outcome by intensification of treatment schedules through introduction of novel induction and combination chemotherapy regimen and altered fractionation regimen, patient tolerance to higher treatment intensities is limited by accompanying side-effects. Combined radioimmunotherapy with cetuximab as well as modern radiotherapy techniques such as intensity-modulated radiotherapy (IMRT) and carbon ion therapy (C12) are able to limit toxicity while maintaining treatment effects. In order to achieve maximum efficacy with yet acceptable toxicity, this sequential phase II trial combines induction chemotherapy with docetaxel, cisplatin, and 5-FU (TPF) followed by radioimmunotherapy with cetuximab as IMRT plus carbon ion boost. We expect this approach to result in increased cure rates with yet manageable accompanying toxicity.
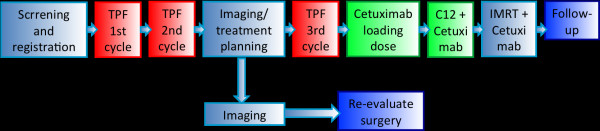
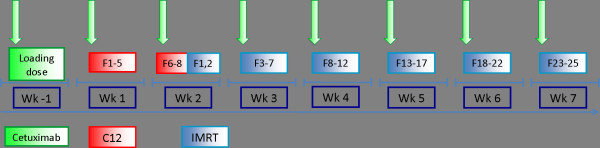
METHODS/DESIGN: The TPF-C-HIT trial is a prospective, mono-centric, open-label, non-randomized phase II trial evaluating efficacy and toxicity of the combined treatment with IMRT/carbon ion boost and weekly cetuximab in 50 patients with histologically proven locally advanced SCCHN following TPF induction chemotherapy. Patients receive 24 GyE carbon ions (8 fractions) and 50 Gy IMRT (2.0 Gy/fraction) in combination with weekly cetuximab throughout radiotherapy. Primary endpoint is locoregional control at 12 months, secondary endpoints are disease-free survival, progression-free survival, overall survival, acute and late radiation effects as well as any adverse events of the treatment as well as quality of life (QoL) analyses.
The primary objective of TPF-C-HIT is to evaluate efficacy and toxicity of cetuximab in combination with combined IMRT/carbon ion therapy following TPF induction in locally advanced SCCHN.
局部晚期头颈部鳞状细胞癌(SCCHN)的长期局部区域控制仍然具有挑战性。近年来,通过引入新的诱导和联合化疗方案以及改变分割方案来加强治疗方案,以提高治疗效果,从而改善了治疗效果,但由于伴随的副作用,患者对更高治疗强度的耐受性有限。联合放射免疫治疗与西妥昔单抗以及现代放射治疗技术,如调强放射治疗(IMRT)和碳离子治疗(C12),能够在保持治疗效果的同时限制毒性。为了在可接受的毒性水平下实现最大疗效,这项序贯 II 期试验将多西紫杉醇、顺铂和 5-FU(TPF)诱导化疗与西妥昔单抗放射免疫治疗相结合,作为 IMRT 加碳离子增强。我们预计这种方法会增加治愈率,同时伴随可管理的毒性。
方法/设计:TPF-C-HIT 试验是一项前瞻性、单中心、开放标签、非随机 II 期试验,评估 TPF 诱导化疗后局部晚期 SCCHN 患者接受 IMRT/碳离子增强联合每周西妥昔单抗治疗的疗效和毒性。患者接受 24 GyE 碳离子(8 个分次)和 50 Gy IMRT(2.0 Gy/分次),并在整个放疗过程中联合每周西妥昔单抗。主要终点是 12 个月时的局部区域控制,次要终点是无病生存率、无进展生存率、总生存率、急性和晚期放射效应以及治疗的任何不良反应以及生活质量(QoL)分析。
TPF-C-HIT 的主要目的是评估 TPF 诱导后在局部晚期 SCCHN 中联合使用西妥昔单抗与联合 IMRT/碳离子治疗的疗效和毒性。