Ossendorf Christian, Steinwachs Matthias R, Kreuz Peter C, Osterhoff Georg, Lahm Andreas, Ducommun Pascal P, Erggelet Christoph
Department of Surgery, Division of Trauma Surgery, University Hospital Zurich, Raemistrasse 100, 8091 Zurich, Switzerland.
Sports Med Arthrosc Rehabil Ther Technol. 2011 May 21;3:11. doi: 10.1186/1758-2555-3-11.
Complex cartilage lesions of the knee including large cartilage defects, kissing lesions, and osteoarthritis (OA) represent a common problem in orthopaedic surgery and a challenging task for the orthopaedic surgeon. As there is only limited data, we performed a prospective clinical study to investigate the benefit of autologous chondrocyte implantation (ACI) for this demanding patient population.
Fifty-one patients displaying at least one of the criteria were included in the present retrospective study: (1.) defect size larger than 10 cm2; (2.) multiple lesions; (3.) kissing lesions, cartilage lesions Outerbridge grade III-IV, and/or (4.) mild/moderate osteoarthritis (OA). For outcome measurements, the International Cartilage Society's International Knee Documentation Committee's (IKDC) questionnaire, as well as the Cincinnati, Tegner, Lysholm and Noyes scores were used. Radiographic evaluation for OA was done using the Kellgren score.
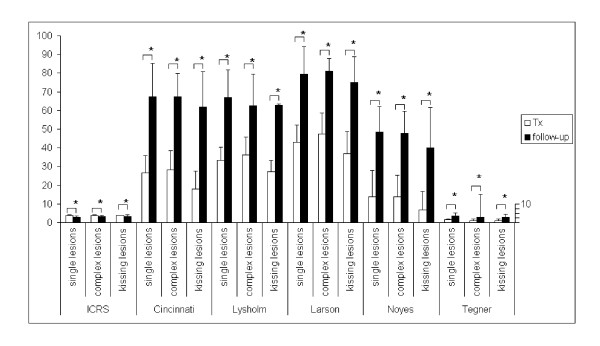
Patient's age was 36 years (13-61), defects size 7.25 (3-17.5) cm2, previous surgical procedures 1.94 (0-8), and follow-up 30 (12-63) months. Instruments for outcome measurement indicated significant improvement in activity, working ability, and sports. Mean ICRS grade improved from 3.8 preoperatively to grade 3 postoperatively, Tegner grade 1.4 enhanced to grade 3.39. The Cincinnati score enhanced from 25.65 to 66.33, the Lysholm score from 33.26 to 64.68, the Larson score from 43.59 to 79.31, and Noyes score from 12.5 to 46.67, representing an improvement from Cincinnati grade 3.65 to grade 2.1. Lysholm grade 4 improved to grade 3.33, and Larson grade 3.96 to 2.78 (Table 1), (p < 0.001). Patients with kissing cartilage lesions had similar results as patients with single cartilage lesions.
Our results suggest that ACI provides mid-term results in patients with complex cartilage lesions of the knee. If long term results will confirm our findings, ACI may be a considered as a valuable tool for the treatment of complex cartilage lesions of the knee.
膝关节复杂软骨损伤,包括大面积软骨缺损、对吻损伤和骨关节炎(OA),是骨科手术中常见的问题,对骨科医生来说是一项具有挑战性的任务。由于相关数据有限,我们进行了一项前瞻性临床研究,以调查自体软骨细胞移植(ACI)对这类高需求患者群体的益处。
本回顾性研究纳入了51例符合至少一项以下标准的患者:(1)缺损面积大于10平方厘米;(2)多处损伤;(3)对吻损伤、Outerbridge III-IV级软骨损伤和/或(4)轻/中度骨关节炎(OA)。采用国际软骨协会国际膝关节文献委员会(IKDC)问卷以及辛辛那提、特格纳、利绍姆和诺伊斯评分进行结果测量。使用凯尔格伦评分对OA进行影像学评估。
患者年龄为36岁(13 - 61岁)。缺损面积7.25(3 - 17.5)平方厘米,既往手术次数1.94(0 - 8次),随访30(12 - 63)个月。结果测量工具显示,患者在活动、工作能力和运动方面有显著改善。国际软骨修复协会(ICRS)平均评分从术前的3.8级提高到术后的3级,特格纳评分从1.4级提高到3.39级。辛辛那提评分从25.65提高到66.33,利绍姆评分从33.26提高到64.68,拉森评分从43.59提高到79.31,诺伊斯评分从12.5提高到46.67,相当于辛辛那提分级从3.65级提高到2.1级。利绍姆分级从4级提高到3.33级,拉森分级从3.96级提高到2.78级(表1),(p < 0.001)。对吻软骨损伤患者的结果与单一软骨损伤患者相似。
我们的结果表明,ACI为膝关节复杂软骨损伤患者提供了中期疗效。如果长期结果能证实我们的发现,ACI可能被视为治疗膝关节复杂软骨损伤的一种有价值的工具。