Department of General Practice/Family Medicine, University of Marburg, 35032 Marburg, Germany.
BMC Fam Pract. 2011 Jun 6;12:45. doi: 10.1186/1471-2296-12-45.
Chest pain is a common complaint and reason for consultation in primary care. Few data exist from a primary care setting whether male patients are treated differently than female patients. We examined whether there are gender differences in general physicians' (GPs) initial assessment and subsequent management of patients with chest pain, and how these differences can be explained
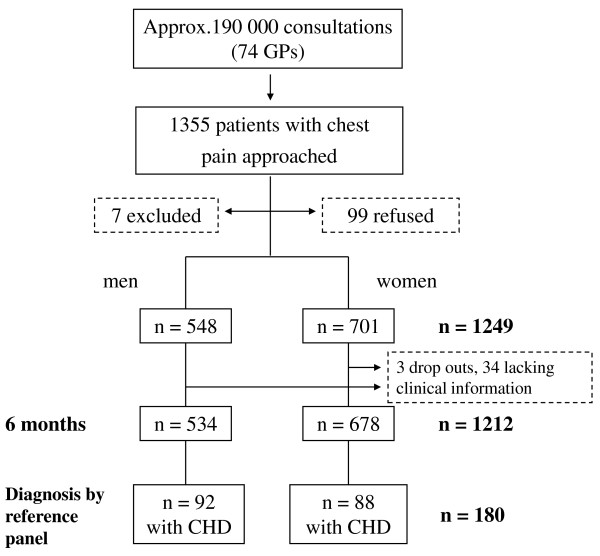
We conducted a prospective study with 1212 consecutive chest pain patients. The study was conducted in 74 primary care offices in Germany from October 2005 to July 2006. After a follow up period of 6 months, an independent interdisciplinary reference panel reviewed clinical data of every patient and decided about the etiology of chest pain at the time of patient recruitment (delayed type-reference standard). We adjusted gender differences of six process indicators for different models.
GPs tended to assume that CHD is the cause of chest pain more often in male patients and referred more men for an exercise test (women 4.1%, men 7.3%, p = 0.02) and to the hospital (women 2.9%, men 6.6%, p < 0.01). These differences remained when adjusting for age and cardiac risk factors but ceased to exist after adjusting for the typicality of chest pain.
While observed gender differences can not be explained by differences in age, CHD prevalence, and underlying risk factors, the less typical symptom presentation in women might be an underlying factor. However this does not seem to result in suboptimal management in women but rather in overuse of services for men. We consider our conclusions rather hypothesis generating and larger studies will be necessary to prove our proposed model.
胸痛是常见的主诉和初级保健咨询的原因。在初级保健环境中,很少有数据表明男性患者的治疗方法是否与女性患者不同。我们研究了全科医生(GP)对胸痛患者的初始评估和后续管理中是否存在性别差异,以及这些差异如何解释。
我们进行了一项前瞻性研究,共纳入了 1212 例连续胸痛患者。该研究于 2005 年 10 月至 2006 年 7 月在德国的 74 个初级保健办公室进行。在 6 个月的随访期后,一个独立的跨学科参考小组审查了每位患者的临床数据,并根据患者招募时(延迟型参考标准)的病因决定胸痛的病因。我们为六个过程指标调整了性别差异的不同模型。
GP 倾向于认为 CHD 是男性胸痛患者的主要病因,并将更多的男性患者转介进行运动试验(女性 4.1%,男性 7.3%,p = 0.02)和住院(女性 2.9%,男性 6.6%,p < 0.01)。在调整年龄和心脏危险因素后,这些差异仍然存在,但在调整胸痛典型性后,这些差异就不存在了。
虽然观察到的性别差异不能用年龄、CHD 患病率和潜在危险因素的差异来解释,但女性胸痛症状不典型可能是一个潜在因素。然而,这似乎并没有导致女性的管理不当,而是导致男性过度使用服务。我们认为我们的结论只是一个假设,需要进行更大规模的研究来证明我们提出的模型。