Pediatric Infectious Diseases, University of Utah, Salt Lake City, Utah, United States of America.
PLoS One. 2011;6(5):e20325. doi: 10.1371/journal.pone.0020325. Epub 2011 May 31.
Community-acquired pneumonia (CAP) is a common childhood infection. CAP complications, such as parapneumonic empyema (PPE), are increasing and are frequently caused by antibiotic-resistant organisms. No clinical guidelines currently exist for management of pediatric CAP and no published data exist about variations in antibiotic prescribing patterns. Our objectives were to describe variation in CAP clinical management for hospitalized children by pediatric infectious disease consultants and to examine associations between recommended antibiotic regimens and local antibiotic resistance levels.
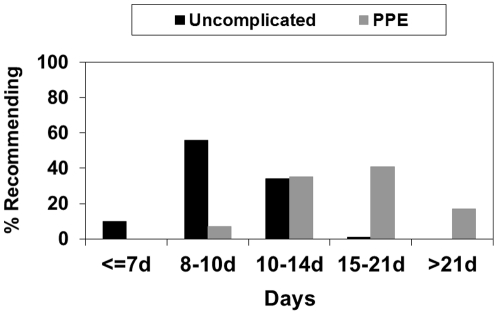
We surveyed pediatric members of the Emerging Infections Network, which consists of 259 pediatric infectious disease physicians. Participants responded regarding their recommended empiric antibiotic regimens for hospitalized children with CAP with and without PPE and their recommendations for duration of therapy. Participants also provided information about the prevalence of penicillin non-susceptible S. pneumoniae and methicillin-resistant S. aureus (MRSA) in their community.
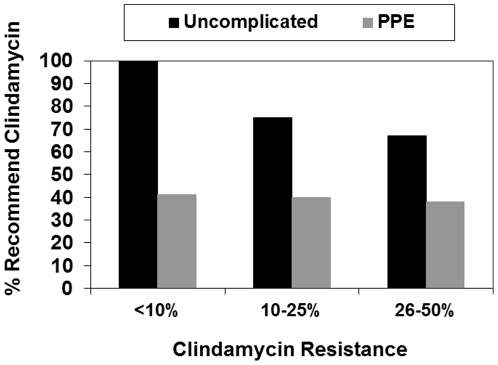
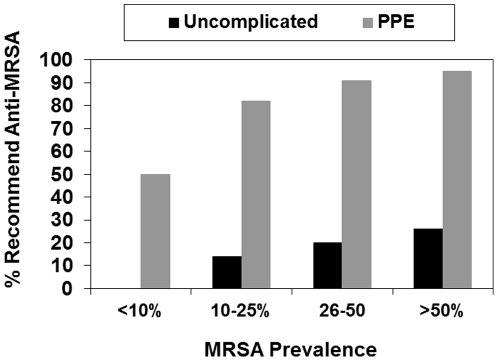
We received 148 responses (57%). For uncomplicated CAP, respondents were divided between recommending beta-lactams alone (55%) versus beta-lactams in combination with another class (40%). For PPE, most recommended a combination of a beta-lactam plus an anti-MRSA agent, however, they were divided between clindamycin (44%) and vancomycin (57%). The relationship between reported antibiotic resistance and empiric regimen was mixed. We found no relationship between aminopenicillin use and prevalence of penicillin non-suscepetible S. pneumoniae or clindamycin use and clindamycin resistance, however, respondents were more likely to recommend an anti-MRSA agent when MRSA prevalence increased.
Substantial variability exists in recommendations for CAP management. Development of clinical guidelines via antimicrobial stewardship programs and dissemination of data about local antibiotic resistance patterns represent opportunities to improve care.
社区获得性肺炎(CAP)是一种常见的儿童感染。CAP 并发症,如肺炎旁胸腔积液(PPE),正在增加,并且通常由抗生素耐药菌引起。目前尚无管理儿科 CAP 的临床指南,也没有关于抗生素处方模式变化的发表数据。我们的目标是描述儿科传染病顾问管理住院儿童 CAP 的临床管理中的差异,并研究推荐的抗生素方案与当地抗生素耐药水平之间的关系。
我们对新兴传染病网络的儿科成员进行了调查,该网络由 259 名儿科传染病医生组成。参与者根据其对住院 CAP 儿童和伴有 PPE 的 CAP 儿童的经验性抗生素治疗方案以及治疗持续时间的建议进行了回答。参与者还提供了有关其社区中青霉素不敏感肺炎链球菌和耐甲氧西林金黄色葡萄球菌(MRSA)流行率的信息。
我们收到了 148 份回复(57%)。对于不复杂的 CAP,大多数受访者推荐单独使用β-内酰胺类药物(55%)或与其他类别联合使用(40%)。对于 PPE,大多数人建议使用β-内酰胺类药物加抗 MRSA 药物联合治疗,但他们在克林霉素(44%)和万古霉素(57%)之间存在分歧。报告的抗生素耐药性与经验性方案之间的关系是混合的。我们发现,青霉素类药物的使用与青霉素不敏感肺炎链球菌的流行率之间没有关系,克林霉素的使用与克林霉素耐药性之间也没有关系,但是当 MRSA 的流行率增加时,受访者更有可能推荐使用抗 MRSA 药物。
CAP 管理的建议存在很大差异。通过抗菌药物管理计划制定临床指南以及传播有关当地抗生素耐药模式的数据代表了改善治疗的机会。