Imaging Science, Proteomics and Genomics Research Group, School of Cancer and Enabling Sciences, University of Manchester, Manchester Academic Health Sciences Centre, Oxford Road, Manchester M13 9PT, UK. james.o'
Br J Cancer. 2011 Jun 28;105(1):139-45. doi: 10.1038/bjc.2011.191. Epub 2011 Jun 14.
There is limited evidence that imaging biomarkers can predict subsequent response to therapy. Such prognostic and/or predictive biomarkers would facilitate development of personalised medicine. We hypothesised that pre-treatment measurement of the heterogeneity of tumour vascular enhancement could predict clinical outcome following combination anti-angiogenic and cytotoxic chemotherapy in colorectal cancer (CRC) liver metastases.
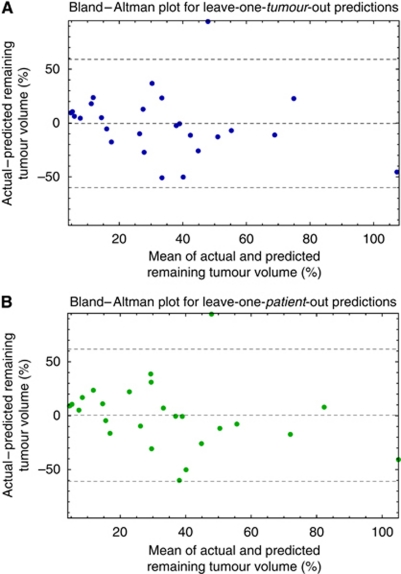
Ten patients with 26 CRC liver metastases had two dynamic contrast-enhanced MRI (DCE-MRI) examinations before starting first-line bevacizumab and FOLFOX-6. Pre-treatment biomarkers of tumour microvasculature were computed and a regression analysis was performed against the post-treatment change in tumour volume after five cycles of therapy. The ability of the resulting linear model to predict tumour shrinkage was evaluated using leave-one-out validation. Robustness to inter-visit variation was investigated using data from a second baseline scan.
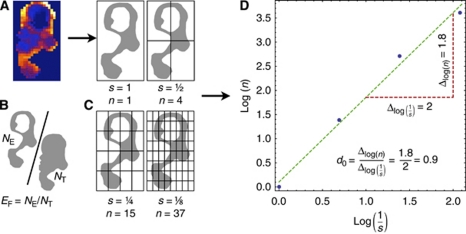
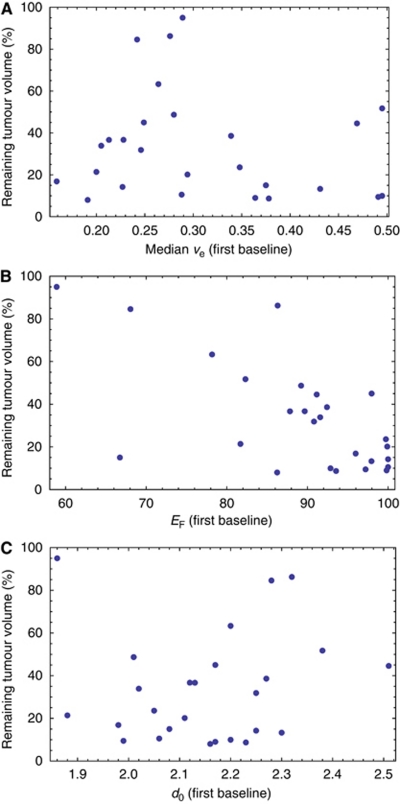
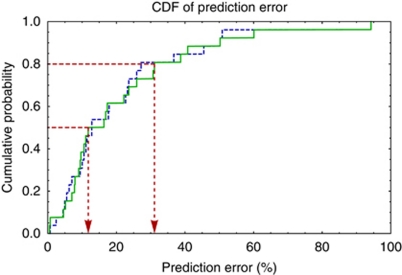
In all, 86% of the variance in post-treatment tumour shrinkage was explained by the median extravascular extracellular volume (v(e)), tumour enhancing fraction (E(F)), and microvascular uniformity (assessed with the fractal measure box dimension, d(0)) (R(2)=0.86, P<0.00005). Other variables, including baseline volume were not statistically significant. Median prediction error was 12%. Equivalent results were obtained from the second scan.
Traditional image analyses may over-simplify tumour biology. Measuring microvascular heterogeneity may yield important prognostic and/or predictive biomarkers.
目前,仅有有限的证据表明影像学生物标志物可以预测后续的治疗反应。此类预后和/或预测性生物标志物将有助于开发个体化医学。我们假设,在开始一线抗血管生成和细胞毒性化疗之前,对肿瘤血管增强异质性的预治疗测量可以预测结直肠癌(CRC)肝转移患者接受联合抗血管生成和细胞毒性化疗后的临床结果。
10 名患者的 26 个 CRC 肝转移灶在开始一线贝伐单抗和 FOLFOX-6 治疗前进行了两次动态对比增强 MRI(DCE-MRI)检查。计算了肿瘤微血管的预治疗生物标志物,并对治疗五个周期后肿瘤体积的变化进行了回归分析。使用留一法验证评估了由此产生的线性模型预测肿瘤缩小的能力。使用第二次基线扫描的数据研究了对访问间变异性的稳健性。
在所有患者中,治疗后肿瘤缩小的 86%的方差由血管外细胞外体积(v(e))、肿瘤增强分数(E(F))和微血管均匀性(用分形测量盒维数(d(0))评估)的中位数解释(R(2)=0.86,P<0.00005)。其他变量,包括基线体积都没有统计学意义。中位数预测误差为 12%。第二次扫描也得到了类似的结果。
传统的图像分析可能过于简化了肿瘤生物学。测量微血管异质性可能产生重要的预后和/或预测性生物标志物。