Haematology-Oncology and Stem Cell Transplantation Unit, National Cancer Institute, Fondazione G. Pascale, IRCCS, Naples, Italy.
Br J Haematol. 2011 Sep;154(5):579-89. doi: 10.1111/j.1365-2141.2011.08786.x. Epub 2011 Jun 28.
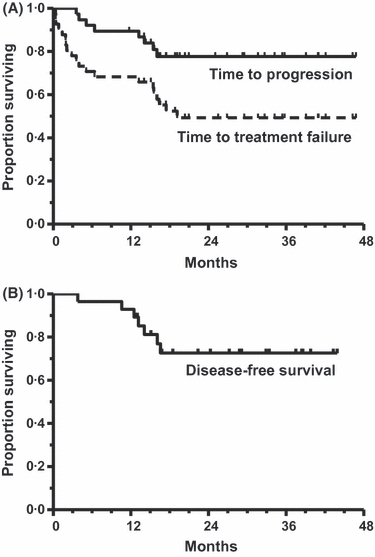
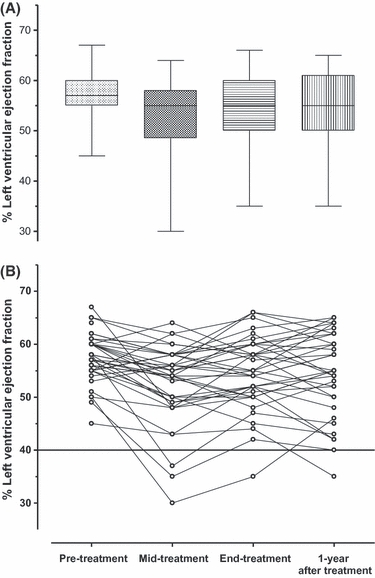
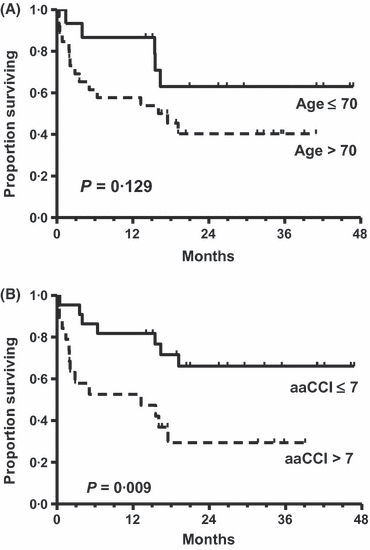
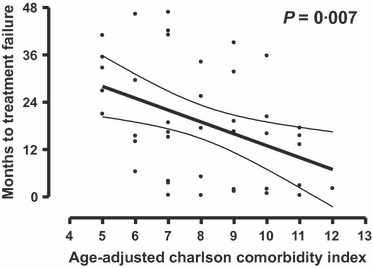
This Phase II study assessed feasibility and efficacy of a biweekly R-COMP-14 regimen (rituximab, cyclophosphamide, non-pegylated liposome-encapsulated doxorubicin, vincristine and prednisone) in untreated elderly patients with poor-risk diffuse large B-cell lymphoma (DLBCL) and moderate to high 'life threat' impact NIA/NCI cardiac comorbidity. A total of 208 courses were delivered, with close cardiac monitoring, to 41 patients (median age: 73years, range: 62-82; 37% >75years) at a median interval of 15·6 (range, 13-29) days; 67% completed all six scheduled courses. Response rate was 73%, with 68% complete responses (CR); 4-year disease-free survival (DFS) and time to treatment failure (TTF) were 72% and 49%, respectively. Failures were due to early death (n=3), therapy discontinuations (no-response n=2; toxicity n=6), relapse (n=6) and death in CR (n=3). Incidence of cardiac grade 3-5 adverse events was 7/41 (17%; 95% confidence interval: 8-31%). Time to progression and overall survival at 4-years were 77% and 67%, respectively. The Age-adjusted Charlson Comorbidity Index (aaCCI) correlated with failures (P=0·007) with patients scoring ≤7 having a longer TTF (66% vs. 29%; P=0·009). R-COMP-14 is feasible and ensures a substantial DFS to poor-risk DLBCL patients who would have been denied anthracycline-based treatment due to cardiac morbidity. The aaCCI predicted both treatment discontinuation rate and TTF.
这项 II 期研究评估了每周两次 R-COMP-14 方案(利妥昔单抗、环磷酰胺、非聚乙二醇化脂质体阿霉素、长春新碱和泼尼松)在未经治疗的老年高危弥漫性大 B 细胞淋巴瘤(DLBCL)和中高危“生命威胁”影响 NIA/NCI 心脏合并症患者中的可行性和疗效。共给予 41 例患者 208 个疗程(中位数年龄:73 岁,范围:62-82;37%>75 岁),中位数间隔为 15.6 天(范围,13-29);67%完成了所有 6 个预定疗程。缓解率为 73%,完全缓解率(CR)为 68%;4 年无疾病生存(DFS)和治疗失败时间(TTF)分别为 72%和 49%。失败的原因是早期死亡(n=3)、治疗中断(无反应 n=2;毒性 n=6)、复发(n=6)和 CR 死亡(n=3)。心脏 3-5 级不良事件发生率为 7/41(17%;95%置信区间:8-31%)。4 年时的进展时间和总生存率分别为 77%和 67%。年龄调整Charlson 合并症指数(aaCCI)与失败相关(P=0.007),评分≤7 的患者 TTF 更长(66% vs. 29%;P=0.009)。R-COMP-14 是可行的,它可以确保高危 DLBCL 患者获得显著的 DFS,这些患者由于心脏合并症而被排除在基于蒽环类药物的治疗之外。aaCCI 预测了治疗中断率和 TTF。