Centre for Infectious Disease and Epidemiology Research School of Health Sciences, University of Cape Town, Observatory, 7925, Cape Town, South Africa.
Eur Respir J. 2012 Jan;39(1):163-71. doi: 10.1183/09031936.00058911. Epub 2011 Jun 30.
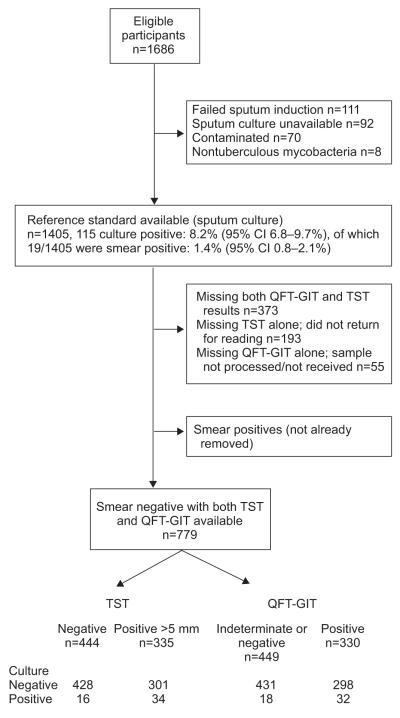
Clinical algorithms for evaluating HIV-infected individuals for tuberculosis (TB) prior to isoniazid preventive therapy (IPT) perform poorly, and interferon-γ release assays (IGRAs) have moderate accuracy for active TB. It is unclear whether, when used as adjunct tests, IGRAs add any clinical discriminatory value for active TB diagnosis in the pre-IPT assessment. 779 sputum smear-negative HIV-infected persons, established on or about to commence combined antiretroviral therapy (ART), were screened for TB prior to IPT. Stepwise multivariable logistic regression was used to develop clinical prediction models. The discriminatory ability was assessed by receiver operator characteristic area under the curve (AUC). QuantiFERON-TB Gold in-tube (QFT-GIT) was evaluated. The prevalence of smear-negative TB by culture was 6.4% (95% CI 4.9-8.4%). Used alone, QFT-GIT and the tuberculin skin test (TST) had comparable performance; the post-test probability of disease based on single negative tests was 3-4%. In a multivariable model, the QFT-GIT test did not improve the ability of a clinical algorithm, which included not taking ART, weight <60 kg, no prior history of TB, any one positive TB symptom/sign (cough ≥ 2 weeks) and CD4+ count <250 cells per mm(3), to discriminate smear-negative culture-positive and -negative TB (72% to 74%; AUC comparison p=0.33). The TST marginally improved the discriminatory ability of the clinical model (to 77%, AUC comparison p=0.04). QFT-GIT does not improve the discriminatory ability of current TB screening clinical algorithms used to evaluate HIV-infected individuals for TB ahead of preventive therapy. Evaluation of new TB diagnostics for clinical relevance should follow a multivariable process that goes beyond test accuracy.
在开始异烟肼预防性治疗 (IPT) 之前,评估 HIV 感染者结核病 (TB) 的临床算法表现不佳,而干扰素-γ释放试验 (IGRAs) 对活动性 TB 具有中等准确性。目前尚不清楚在 IPT 评估中,作为辅助检测,IGRAs 是否会为活动性 TB 诊断提供任何临床鉴别价值。779 例痰涂片阴性的 HIV 感染者,在开始或即将开始联合抗逆转录病毒治疗 (ART) 时,在开始 IPT 之前进行了 TB 筛查。采用逐步多变量逻辑回归方法建立临床预测模型。通过受试者工作特征曲线下面积 (AUC) 评估鉴别能力。评估了 QuantiFERON-TB Gold in-tube (QFT-GIT)。培养物中涂片阴性 TB 的患病率为 6.4%(95%CI 4.9-8.4%)。单独使用时,QFT-GIT 和结核菌素皮肤试验 (TST) 具有相当的性能;根据单次阴性检测,疾病的后验概率为 3-4%。在多变量模型中,QFT-GIT 检测并未改善包含未接受 ART、体重<60kg、无既往 TB 史、任何一个阳性 TB 症状/体征(咳嗽≥2 周)和 CD4+计数<250 个细胞/mm3 的临床算法对涂片阴性培养阳性和阴性 TB 的鉴别能力(72%至 74%;AUC 比较 p=0.33)。TST 略微提高了临床模型的鉴别能力(至 77%,AUC 比较 p=0.04)。QFT-GIT 不能提高当前用于在预防性治疗前评估 HIV 感染者 TB 的 TB 筛查临床算法的鉴别能力。对新的 TB 诊断方法进行临床相关性评估应遵循一个多变量过程,该过程不仅要评估测试准确性。