Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD 21231, USA.
Mod Pathol. 2011 Nov;24(11):1511-20. doi: 10.1038/modpathol.2011.111. Epub 2011 Jul 8.
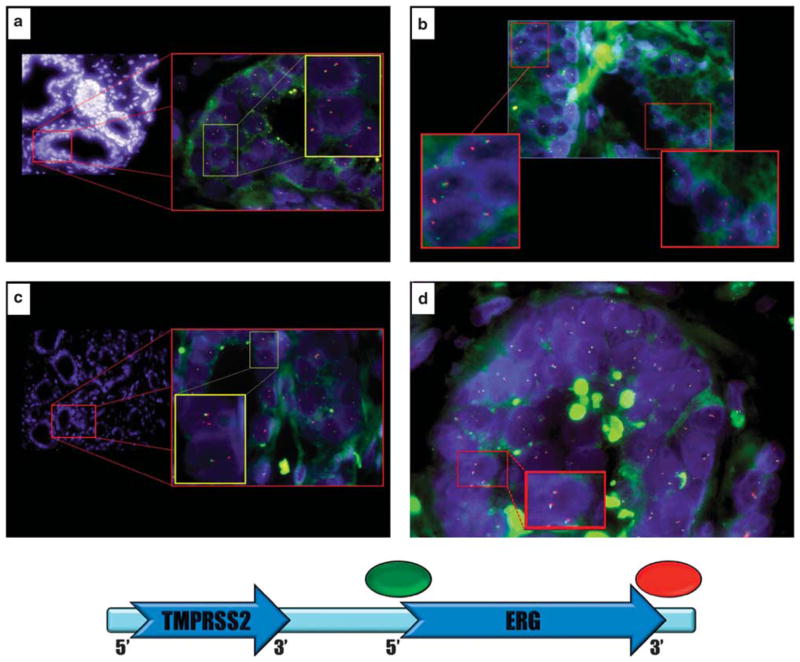
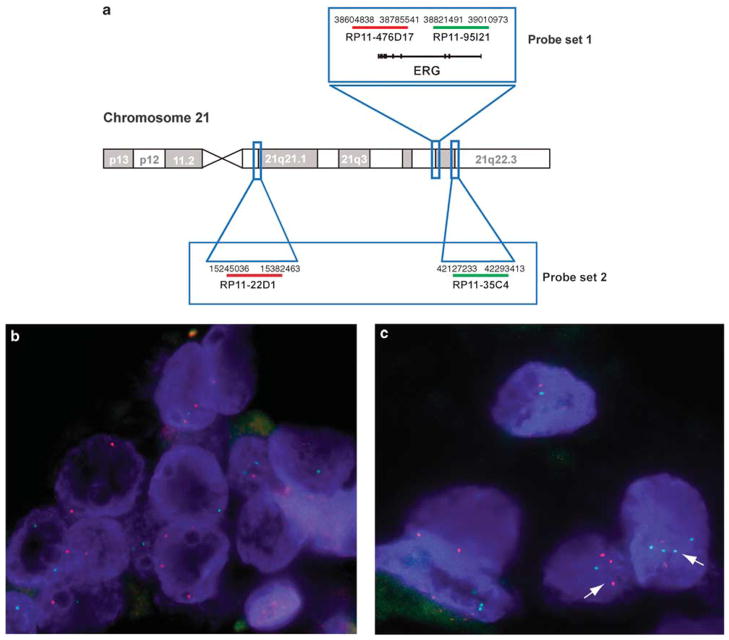
The role of TMPRSS2-ERG gene fusion in prostate cancer prognostication remains controversial. We evaluated the prognostic role of TMPRSS2-ERG fusion using fluorescence in situ hybridization analysis in a case-control study nested in The Johns Hopkins retropubic radical prostatectomy cohort. In all, 10 tissue microarrays containing paired tumors and normal tissues obtained from 172 cases (recurrence) and 172 controls (non-recurrence) matched on pathological grade, stage, race/ethnicity, and age at the time of surgery were analyzed. All radical prostatectomies were performed at our institution between 1993 and 2004. Recurrence was defined as biochemical recurrence, development of clinical evidence of metastasis, or death from prostate carcinoma. Each tissue microarray spot was scored for the presence of TMPRSS2-ERG gene fusion and for ERG gene copy number gains. The odds ratio of recurrence and 95% confidence intervals were estimated from conditional logistic regression. Although the percentage of cases with fusion was slightly lower in cases than in controls (50 vs 57%), the difference was not statistically significant (P=0.20). The presence of fusion due to either deletion or split event was not associated with recurrence. Similarly, the presence of duplicated ERG deletion, duplicated ERG split, or ERG gene copy number gain with a single ERG fusion was not associated with recurrence. ERG gene polysomy without fusion was significantly associated with recurrence (odds ratio 2.0, 95% confidence interval 1.17-3.42). In summary, TMPRSS2-ERG fusion was not prognostic for recurrence after retropubic radical prostatectomy for clinically localized prostate cancer, although men with ERG gene copy number gain without fusion were twice more likely to recur.
TMPRSS2-ERG 基因融合在前列腺癌预后中的作用仍存在争议。我们通过荧光原位杂交分析,在约翰霍普金斯耻骨后前列腺切除术队列的病例对照研究中评估了 TMPRSS2-ERG 融合的预后作用。总共分析了 10 个组织微阵列,其中包含 172 例(复发)和 172 例(非复发)配对肿瘤和正常组织,这些组织在病理分级、分期、种族/民族和手术时的年龄上相匹配。所有前列腺根治术均于 1993 年至 2004 年在我们机构进行。复发定义为生化复发、出现临床转移证据或死于前列腺癌。每个组织微阵列点均对 TMPRSS2-ERG 基因融合和 ERG 基因拷贝数增加进行评分。复发的比值比和 95%置信区间通过条件逻辑回归估计。尽管病例中融合的百分比略低于对照(50%比 57%),但差异无统计学意义(P=0.20)。由于缺失或分裂事件导致的融合存在与复发无关。同样,存在 ERG 缺失的重复、ERG 分裂的重复或单个 ERG 融合的 ERG 基因拷贝数增加与复发无关。无融合的 ERG 基因多倍体与复发显著相关(比值比 2.0,95%置信区间 1.17-3.42)。总之,在耻骨后前列腺切除术治疗局限性前列腺癌后,TMPRSS2-ERG 融合与复发无关,尽管无融合的 ERG 基因拷贝数增加的男性复发的可能性增加了两倍。