Division of Epidemiology and Public Health, The University of Nottingham, Nottingham City Hospital, Nottingham, UK.
Gut. 2012 Apr;61(4):514-20. doi: 10.1136/gutjnl-2011-300186. Epub 2011 Jul 13.
Inequalities in health are well recognized in cardiovascular disease and cancer, but in comparison, we have minimal understanding for upper gastrointestinal bleeding. Since furthering our understanding of such inequality signposts preventable disease, we investigated in detail the association between upper gastrointestinal bleeding and socioeconomic status.
Population-based cohort study.
All English National Health Service hospitals.
English adult population, 1 January 2001 to 31 December 2007.
Deprivation scores defined according to quintiles of neighbourhood areas ranked by the Indices of Multiple Deprivation for England 2007.
Rates of all adult admissions coded with a primary diagnosis of upper gastrointestinal bleed were analysed by deprivation quintile and adjusted for age, sex, region and year using Poisson regression.
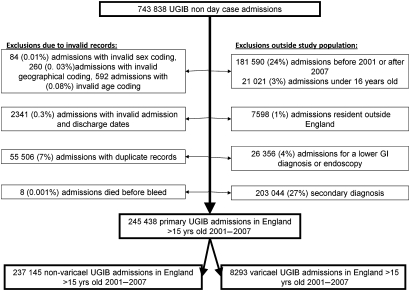
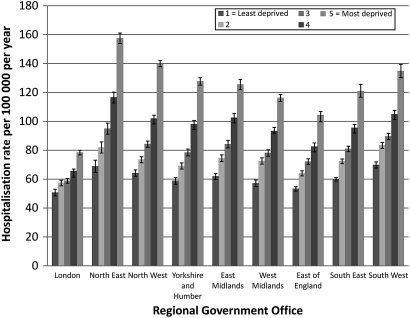
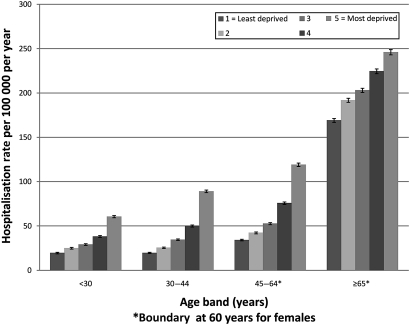
The annual hospitalization rate for non-variceal haemorrhage was 84.6 per 100,000 population (95% CI 83.5 to 84.1; n=237,145), and for variceal haemorrhage, it was 2.83 per 100,000 population (95% CI 2.87 to 2.99; n=8291). There was a twofold increase in the hospitalization rate ratio for non-variceal haemorrhage from the most deprived areas compared to the least deprived (2.00, 95% CI 1.98 to 2.03). The ratio for variceal haemorrhage was even more pronounced (2.49, 95% CI 2.32 to 2.67). Inequality increased over the study period (non-variceal p<0.0001, variceal p=0.0068), and adjusting for age and sex increased the disparity between deprived and affluent areas. Case fatality did not have a similar socioeconomic gradient.
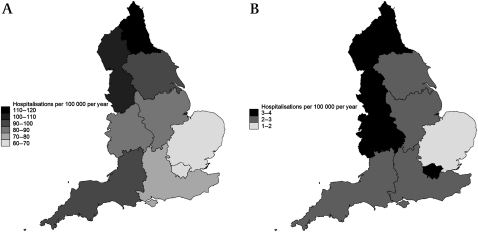
Both variceal and non-variceal haemorrhage hospitalization rates increased with deprivation, and there was a similar gradient in all areas of the country and in all age bands. The existence of such a steep gradient suggests that there are opportunities to reduce hospitalizations down to the low rates seen in the most affluent, and thus, there is the potential to prevent almost 10,000 admissions and over 1000 deaths a year.
心血管疾病和癌症的健康不平等现象已得到广泛认识,但相比之下,我们对上消化道出血的认识还很有限。由于进一步了解这种不平等现象可以发现可预防的疾病,因此我们详细研究了上消化道出血与社会经济地位之间的关系。
基于人群的队列研究。
所有英国国民保健署医院。
2001 年 1 月 1 日至 2007 年 12 月 31 日期间的英国成年人群。
根据英格兰 2007 年多因素剥夺指数对街区进行五分位数排序,根据街区定义贫困评分。
按贫困五分位组分析了所有成年人因上消化道出血而住院的诊断率,采用泊松回归模型,根据年龄、性别、地区和年份进行了调整。非静脉曲张性出血的年住院率为 84.6/100000 人(95%CI83.5-84.1;n=237145),静脉曲张性出血的年住院率为 2.83/100000 人(95%CI2.87-2.99;n=8291)。与最贫困地区相比,非静脉曲张性出血的住院率比值增加了两倍(2.00,95%CI1.98-2.03)。静脉曲张性出血的比值更为明显(2.49,95%CI2.32-2.67)。研究期间不平等现象加剧(非静脉曲张性 p<0.0001,静脉曲张性 p=0.0068),并且根据年龄和性别调整后,贫困地区和富裕地区之间的差距进一步扩大。病死率没有类似的社会经济梯度。
静脉曲张性和非静脉曲张性出血的住院率随贫困程度而增加,在全国所有地区和所有年龄组中都存在类似的梯度。这种陡峭梯度的存在表明,有机会将住院率降低到最富裕地区的低水平,因此每年可减少近 10000 次住院和 1000 多例死亡。