Buhagiar Luana, Cassar Olivia A, Brincat Mark P, Buttigieg George G, Inglott Anthony Serracino, Adami Maurice Zarb, Azzopardi Lilian M
Department of Pharmacy, Faculty of Medicine and Surgery, University of Malta, Msida, Malta.
J Anaesthesiol Clin Pharmacol. 2011 Apr;27(2):185-91. doi: 10.4103/0970-9185.81822.
Ideally, the intensity of postoperative pain should be predicted so as to customize analgesia. The objective of this study was to investigate whether preoperative electrical and pressure pain assessment can predict post-caesarean section pain and analgesic requirement.
A total of 65 subjects scheduled for elective caesarean section, who gave written informed consent, were studied. Preoperatively, PainMatcher(®) was used to evaluate electrical pain threshold, while manual PainTest™ FPN 100 Algometer and digital PainTest™ FPX 25 Algometer determined pressure pain threshold and tolerance. Postoperatively, numerical rating scales were used to assess pain at regular time intervals. Patients received intramuscular pethidine (100mg, 6 hourly), rectal diclofenac (100mg, 12 hourly), and oral paracetamol (1g, p.r.n.) for pain relief. Statistical analysis was conducted using PASW Statistics 18 software.
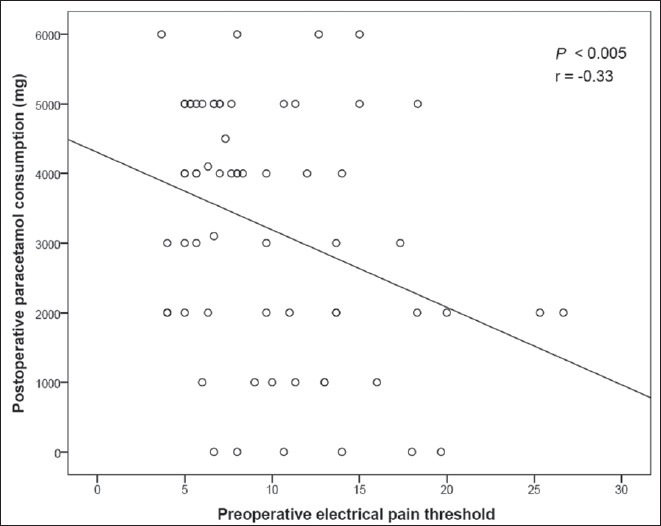
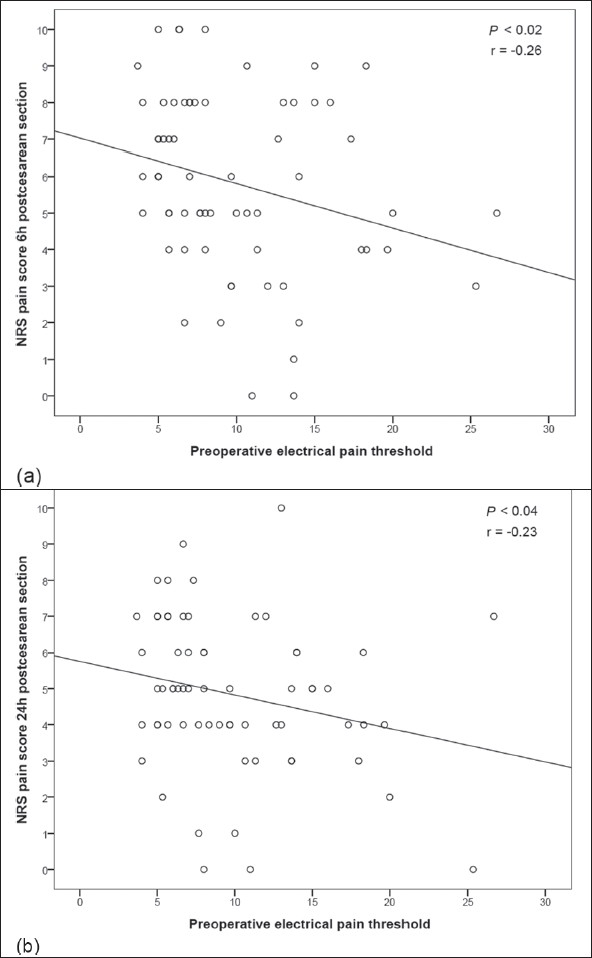
Preoperative electrical pain threshold correlated significantly with post-caesarean pain scores at 6 and 24 hours (r = -0.26, P < 0.02; r = -0.23, P < 0.04, respectively), and with the quantity of paracetamol consumed by the patient within 48 hours of surgery (r = -0.33, P < 0.005). Preoperative pressure pain tolerance measured by PainTest™ FPX 25 Algometer was significantly correlated with pain scores 6 hours postsurgery (r = -0.21, P < 0.05). Pain scores 6 hours post-caesarean section correlated significantly with anesthesia-general or spinal (F = 4.22, v(1) = 1, v(2) = 63, P < 0.05).
The predictive methods proposed may aid in identifying patients at greater risk for postoperative pain. Electrical pain threshold could be useful in personalizing the postoperative analgesic protocol.
理想情况下,应预测术后疼痛强度以便定制镇痛方案。本研究的目的是调查术前电刺激和压力疼痛评估是否能够预测剖宫产术后疼痛及镇痛需求。
共研究了65例计划进行择期剖宫产且签署书面知情同意书的受试者。术前,使用PainMatcher(®)评估电刺激疼痛阈值,同时使用手动PainTest™ FPN 100压力痛觉计和数字PainTest™ FPX 25压力痛觉计测定压力疼痛阈值和耐受性。术后,使用数字评分量表在定期时间间隔评估疼痛。患者接受肌肉注射哌替啶(100mg,每6小时一次)、直肠给予双氯芬酸(100mg,每12小时一次)以及口服对乙酰氨基酚(1g,必要时)以缓解疼痛。使用PASW Statistics 18软件进行统计分析。
术前电刺激疼痛阈值与剖宫产术后6小时和24小时的疼痛评分显著相关(分别为r = -0.26,P < 0.02;r = -0.23,P < 0.04),并且与患者在术后48小时内消耗的对乙酰氨基酚量相关(r = -0.33,P < 0.005)。使用PainTest™ FPX 25压力痛觉计测量的术前压力疼痛耐受性与术后6小时的疼痛评分显著相关(r = -0.21,P < 0.05)。剖宫产术后6小时的疼痛评分与全身麻醉或脊髓麻醉显著相关(F = 4.22,v(1) = 1,v(2) = 63,P < 0.05)。
所提出的预测方法可能有助于识别术后疼痛风险较高的患者。电刺激疼痛阈值可用于个性化术后镇痛方案。