Pederson Aaron W, Salama Joseph K, Haraf Daniel J, Witt Mary Ellen, Stenson Kerstin M, Portugal Louis, Seiwert Tanguy, Villaflor Victoria M, Cohen Ezra E W, Vokes Everett E, Blair Elizabeth A
Department of Radiation Oncology, Memorial University Medical Center, 4700 Waters Avenue, Savannah, GA 31404, USA.
Head Neck Oncol. 2011 Jul 26;3:31. doi: 10.1186/1758-3284-3-31.
To report the outcomes of patients with locoregionally advanced and high- risk salivary gland malignancies treated with surgery followed by adjuvant chemoradiotherapy.
From 09/1991 - 06/2007, 24 high-risk salivary gland cancer patients were treated with surgery, followed by adjuvant chemoradiotherapy for high-risk pathologic features including, perineural involvement, nodal involvement, positive margins, or T3/T4 tumors. Chemoradiotherapy was delivered for 4-6 alternating week cycles: the most common regimen, TFHX, consisted of 5 days paclitaxel (100 mg/m² on d1), infusional 5-fluorouracil (600 mg/m²/d × 5d), hydroxyurea (500 mg PO BID), and 1.5 Gy twice daily irradiation followed by a 9-day break without treatment.
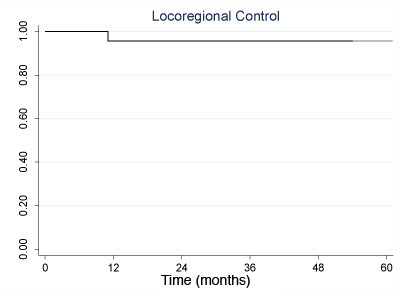
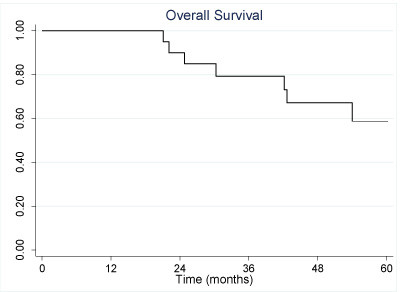
Median follow-up was 42 months. The parotid gland was more frequently involved (n = 17) than minor (n = 4) or submandibular (n = 3) glands. The median radiation dose was 65 Gy (range 55-68 Gy). Acute treatment related toxicity included 46% grade 3 mucositis and 33% grade 3 hematologic toxicity. Six patients required feeding tubes during treatment. One patient progressed locally, 8 patients progressed distantly, and none progressed regionally. Five-year locoregional progression free survival was 96%. The 3 and 5 year overall survival was 79% and 59%, respectively. Long-term complications included persistent xerostomia (n = 5), esophageal stricture requiring dilatation (n = 1), and tempromandibular joint syndrome (n = 1).
Surgical resection followed by adjuvant chemoradiotherapy results in promising locoregional control for high-risk salivary malignancy patients.
报告局部区域晚期和高危涎腺恶性肿瘤患者接受手术加辅助放化疗后的治疗结果。
1991年9月至2007年6月,24例高危涎腺癌患者接受了手术治疗,随后因包括神经周围侵犯、淋巴结受累、切缘阳性或T3/T4肿瘤等高风险病理特征接受辅助放化疗。放化疗为期4 - 6个交替周周期:最常用的方案TFHX包括5天的紫杉醇(第1天100mg/m²)、持续输注5 - 氟尿嘧啶(600mg/m²/天×5天)、羟基脲(口服500mg,每日两次),以及每日两次1.5Gy照射,随后休息9天不进行治疗。
中位随访时间为42个月。腮腺受累(n = 17)比小涎腺(n = 4)或下颌下腺(n = 3)更常见。中位放射剂量为65Gy(范围55 - 68Gy)。急性治疗相关毒性包括46%的3级黏膜炎和33%的3级血液学毒性。6例患者在治疗期间需要鼻饲管。1例患者局部进展,8例患者远处进展,无区域进展。5年局部区域无进展生存率为96%。3年和5年总生存率分别为79%和59%。长期并发症包括持续性口干(n = 5)、需要扩张的食管狭窄(n = 1)和颞下颌关节综合征(n = 1)。
手术切除加辅助放化疗对高危涎腺恶性肿瘤患者的局部区域控制效果良好。