Schneider Uwe, Sumila Marcin, Robotka Judith
Radiotherapy Hirslanden AG, Institute for Radiotherapy, Rain 34, 5001 Aarau, Switzerland.
Theor Biol Med Model. 2011 Jul 26;8:27. doi: 10.1186/1742-4682-8-27.
Most information on the dose-response of radiation-induced cancer is derived from data on the A-bomb survivors. Since, for radiation protection purposes, the dose span of main interest is between zero and one Gy, the analysis of the A-bomb survivors is usually focused on this range. However, estimates of cancer risk for doses larger than one Gy are becoming more important for radiotherapy patients. Therefore in this work, emphasis is placed on doses relevant for radiotherapy with respect to radiation induced solid cancer.
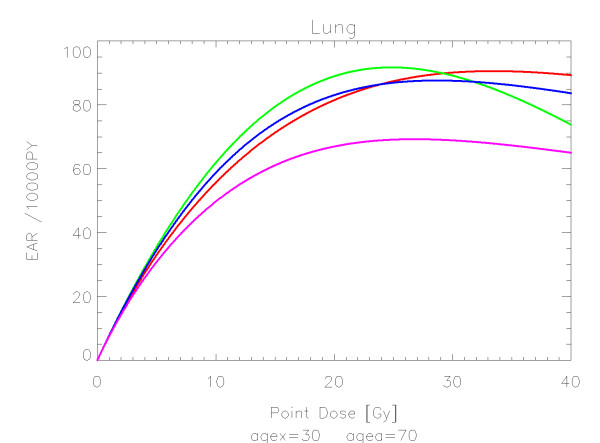
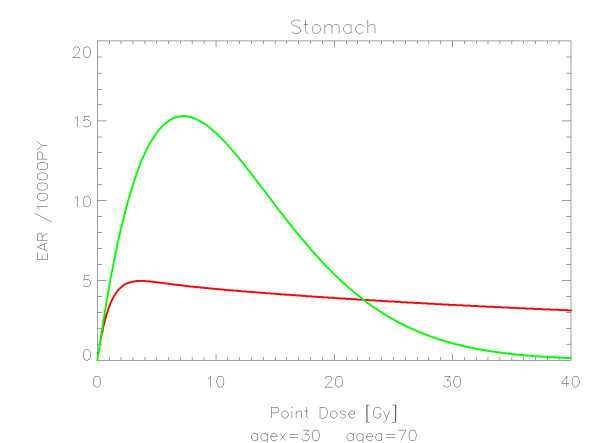
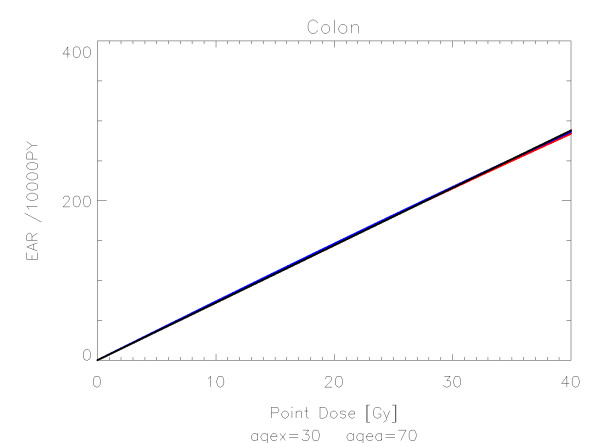
For various organs and tissues the analysis of cancer induction was extended by an attempted combination of the linear-no-threshold model from the A-bomb survivors in the low dose range and the cancer risk data of patients receiving radiotherapy for Hodgkin's disease in the high dose range. The data were fitted using organ equivalent dose (OED) calculated for a group of different dose-response models including a linear model, a model including fractionation, a bell-shaped model and a plateau-dose-response relationship.
The quality of the applied fits shows that the linear model fits best colon, cervix and skin. All other organs are best fitted by the model including fractionation indicating that the repopulation/repair ability of tissue is neither 0 nor 100% but somewhere in between. Bone and soft tissue sarcoma were fitted well by all the models. In the low dose range beyond 1 Gy sarcoma risk is negligible. For increasing dose, sarcoma risk increases rapidly and reaches a plateau at around 30 Gy.
In this work OED for various organs was calculated for a linear, a bell-shaped, a plateau and a mixture between a bell-shaped and plateau dose-response relationship for typical treatment plans of Hodgkin's disease patients. The model parameters (α and R) were obtained by a fit of the dose-response relationships to these OED data and to the A-bomb survivors. For any three-dimensional inhomogenous dose distribution, cancer risk can be compared by computing OED using the coefficients obtained in this work.
关于辐射诱发癌症剂量反应的大多数信息来源于原子弹爆炸幸存者的数据。出于辐射防护目的,主要关注的剂量范围在零至1 Gy之间,因此对原子弹爆炸幸存者的分析通常聚焦于该范围。然而,对于放疗患者而言,大于1 Gy剂量的癌症风险估计变得愈发重要。因此,在本研究中,重点关注与放疗相关的辐射诱发实体癌剂量。
对于各种器官和组织,通过尝试将低剂量范围原子弹爆炸幸存者的线性无阈模型与高剂量范围霍奇金病放疗患者的癌症风险数据相结合,扩展了癌症诱发分析。使用针对一组不同剂量反应模型计算的器官等效剂量(OED)对数据进行拟合,这些模型包括线性模型、包含分次照射的模型、钟形模型和平坦剂量反应关系模型。
所应用拟合的质量表明,线性模型对结肠、宫颈和皮肤的拟合最佳。所有其他器官由包含分次照射的模型拟合效果最佳,这表明组织的再增殖/修复能力既不是0也不是100%,而是介于两者之间。所有模型对骨肉瘤和软组织肉瘤的拟合效果都很好。在超过1 Gy的低剂量范围内,肉瘤风险可忽略不计。随着剂量增加,肉瘤风险迅速上升,并在约30 Gy时达到平台期。
在本研究中,针对霍奇金病患者的典型治疗计划,计算了线性、钟形、平坦以及钟形和平坦剂量反应关系混合模型下各种器官的OED。通过将剂量反应关系拟合到这些OED数据以及原子弹爆炸幸存者数据,获得了模型参数(α和R)。对于任何三维非均匀剂量分布,可使用本研究中获得的系数计算OED来比较癌症风险。