Department of Clinical Pharmacokinetics and Pharmacodynamics, School of Medicine, Keio University, Tokyo, 160-8582, Japan.
Eur J Clin Pharmacol. 2012 Jan;68(1):39-53. doi: 10.1007/s00228-011-1095-3. Epub 2011 Jul 28.
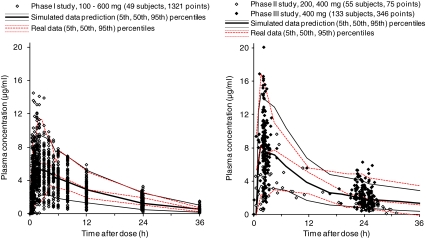
Garenoxacin, a novel des-F(6)-quinolone, possesses potent antibacterial activity against infectious pathogens in the respiratory tract. Population pharmacokinetic/pharmacodynamic (PK/PD) modeling and Monte Carlo simulations were used to optimize garenoxacin dosage regimens.
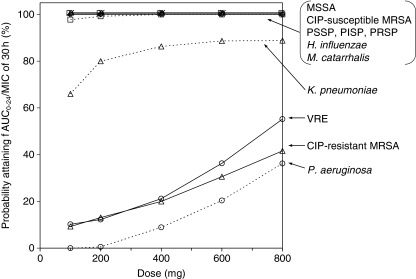
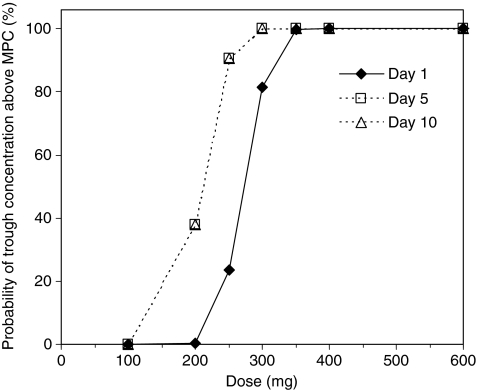
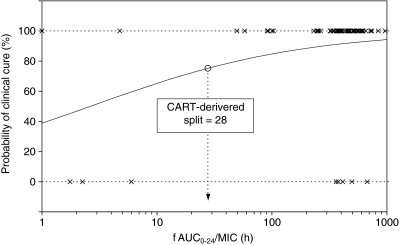
At the end of phase II stage, the clinical dose of garenoxacin was predicted to be 400 mg once daily by the interim PK/PD analysis using phase I and phase II clinical data. The criteria used to determine an optimal dose were (1) the target attainment of the area under the unbound concentration-time curve divided by the minimum inhibitory concentration (fAUC₀₋₂₄/MIC ratio) and (2) the maintenance of a trough concentration above the mutant prevention concentration. In a confirmatory phase III study, garenoxacin was administered 400 mg once daily to 136 patients infected with mild or moderate chronic respiratory diseases.
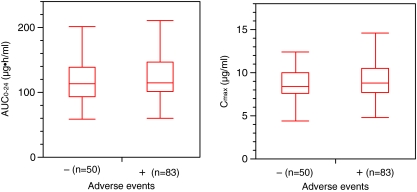
Logistic regression analysis showed that fAUC₀₋₂₄/MIC ratio was a significant variable that predicted clinical response (p = 0.0164). Of all subjects, 92.4% reached the target value of fAUC₀₋₂₄/MIC ratio > 30 h, and the clinical efficacy rate of this population was 91.8%. On the other hand, there was no significant relationship between exposure values (AUC₀₋₂₄ and maximum concentration) and the incidence of adverse events by the Mann-Whitney test.
The antimicrobial efficacy of the actual phase III study was consistent with the expectation from the Monte Carlo PD simulation. We were able to show that the optimal garenoxacin dosage regimens were successfully determined using prospective population PK/PD analysis and clinical trial simulations.
加雷沙星是一种新型的去 F(6)-喹诺酮类药物,对呼吸道感染病原体具有强大的抗菌活性。本研究采用群体药代动力学/药效学(PK/PD)模型和蒙特卡罗模拟来优化加雷沙星的给药方案。
在 II 期临床试验结束时,通过 I 期和 II 期临床试验数据的中期 PK/PD 分析,预测加雷沙星的临床剂量为 400 mg 每日 1 次。确定最佳剂量的标准为(1)未结合浓度-时间曲线下面积与最低抑菌浓度的比值(fAUC₀₋₂₄/MIC 比值)的目标值和(2)谷浓度维持在突变预防浓度之上。在一项确证性 III 期研究中,136 例患有轻度或中度慢性呼吸道疾病的患者接受了每日 400 mg 加雷沙星治疗。
逻辑回归分析表明,fAUC₀₋₂₄/MIC 比值是预测临床反应的显著变量(p=0.0164)。所有患者中有 92.4%达到了 fAUC₀₋₂₄/MIC 比值>30 h 的目标值,该人群的临床疗效率为 91.8%。另一方面,通过曼-惠特尼检验,暴露值(AUC₀₋₂₄和最大浓度)与不良事件的发生率之间没有显著关系。
实际 III 期研究的抗菌疗效与蒙特卡罗 PD 模拟的预期一致。我们能够证明,通过前瞻性的群体 PK/PD 分析和临床试验模拟,可以成功确定加雷沙星的最佳给药方案。